
Health Reports
Sex differences in COVID-19 deaths in the early months of the pandemic in Canada: An examination with an immigration lens
by Edward Ng

DOI: https://www.doi.org/10.25318/82-003-x202301100001-eng
Abstract
Background
At the onset of the COVID-19 pandemic, there was an overrepresentation of males in COVID‑19 deaths worldwide, with Canada reporting more female COVID-19 deaths. This paper examines the overrepresentation of female COVID-19 deaths in Canada, with an immigration lens.
Data and methods
Data were extracted from the COVID-19 Sex-Disaggregated Data Tracker to compare the sex distribution of COVID-19 deaths in Canada with that of other countries. A linkage of deaths to the Longitudinal Immigration Database (IMDB) allows for the comparison of sex-specific COVID-19 death rates by immigrant status for age and geography, as well as by major employment sector among immigrants, using the tax data from the IMDB.
Results
While there were proportionately more female than male COVID-19 deaths in Canada in the early months of the pandemic, this trend was mainly a phenomenon among non-immigrants aged 85 and older. In addition, COVID-19-specific death rates for males were higher than those for females across age groups by immigrant status, except for those aged 85 and older among the non-immigrant population. Among immigrants, the death rate among health care and social assistance workers was higher among males than among females (10.7 vs. 2.9 per 100,000 population). The initially observed overrepresentation of female COVID-19 deaths to male COVID-19 deaths in Canada evened out in the summer of 2021.
Interpretation
The higher proportion of female COVID-19 deaths was likely related to the high concentration of COVID‑19 deaths in long-term care facilities, where a lower institutionalization rate for immigrants had been observed. Since the implementation of vaccination targeting long-term care facility residents in Canada, the overrepresentation of female COVID-19 deaths ceased.
Keywords
COVID-19, sex difference, immigration, long-term care residents, international comparison
Authors
Edward Ng is with the Health Analysis Division, Analytical Studies and Modelling Branch, Statistics Canada.
What is already known on this subject?
- The higher proportion of male deaths observed during the COVID-19 pandemic is a global phenomenon, but the reverse is true in Canada, where the proportion of female COVID-19 deaths was higher at the onset of the pandemic. By immigrant status, however, overrepresentation of female COVID-19 deaths was observed among non-immigrants but not among immigrants.
- More than 80% of COVID-19 deaths at the onset of the pandemic in Canada occurred in long-term care facilities, compared with an average of 38% in other Organisation for Economic Co operation and Development countries.
What does this study add?
- The overrepresentation of female COVID-19 deaths was observed only among those aged 85 and older, especially for non-immigrants. Age-specific death rates were higher for males than females in all age groups, except for those aged 85 and older among non-immigrants.
- The overrepresentation of female COVID-19 deaths among non-immigrants was sustained until early 2021 and could be related to their higher institutionalization rate compared with their immigrant counterparts. Female overrepresentation evened out by mid-2021, when long-term care facility residents were prioritized to receive COVID-19 vaccinations, a measure that resulted in a high reduction of deaths.
- The COVID-19 death rate among immigrant workers was higher for males compared than for females in the health care and social assistance field, a sector where immigrant females were highly concentrated.
Introduction
The COVID-19 pandemic has revealed the vulnerability of certain population groups, such as the elderly and those who have pre-existing co-morbid health conditions (e.g., obesity and diabetes) or are immunocompromised, as being at a high risk of COVID-19 infection and death.Note 1 However, sex also emerged to be a significant risk factor as epidemiological findings revealed higher morbidity and mortality rates in males compared with females worldwide.Note 2 A meta-analysis of 3,111,714 reported global cases shows that male patients were almost three times more likely to require intensive care and had higher odds of death compared with female patients.Note 3 The observed male overrepresentation in COVID-19 mortality impacts seems to be associated with biological and situational factors, which include gender-related social norms, behaviours, and sex-based immunological factors.Note 4, Note 5, Note 6 Also, the prevalence of COVID-19 mortality risk factors, such as diabetes, cancer and smoking, was higher among males than among females in Canada.Note 7 The higher proportion of male COVID-19 deaths observed during the pandemic is a global phenomenon.
Canada may be an exception to the global overrepresentation of COVID-19 deaths in males. Based on a Public Health Agency of Canada (PHAC) report,Note 8 despite emerging international consensus of a higher proportion of males experiencing severe illness and death outcomes related to COVID-19, in Canada during the first few months of the pandemic, females represented a larger proportion of confirmed deaths. This unique sex difference pattern must be monitored and explained. According to the PHAC report, as of June 10, 2020, sex-disaggregated data for COVID‑19‑related deaths in the 30 countries with the most confirmed cases of COVID-19 deaths showed that while the male-to-female ratio of confirmed COVID-19 deaths varied by country, an overrepresentation of male COVID-19 deaths was observed for many of these countries. Only Canada and Finland had a male-to-female ratio markedly under 1, which showed more female than male COVID-19 deaths. Specifically, Canada and Finland had the lowest ratios (below 0.90) compared with the Netherlands, which had the highest male-to-female ratio of deaths (more than 2). Analyses of provisional death data in Canada from March to August 2020 confirmed that there were indeed more female than male COVID-19 deaths in Canada overall. However, additional linkages of death data to the Longitudinal Immigration Database (IMDB) show there were more male COVID-19 deaths than female COVID‑19 deaths among immigrants.Note 9 Specifically, COVID-19 deaths among immigrants in Canada were more frequent among males (55%). Conversely, for COVID-19 deaths among non-immigrants, more than half were females (54%).
Existing plausible explanations for the overrepresentation of female COVID-19 deaths in Canada include the sex-based age distribution, long-term care facility resident distribution, and female frontline health workforce distribution.Note 8 While information on long-term care facility resident distribution is a big data gap in the national statistical system in Canada, efforts are being made to fill it. The data available in this study allow for the evaluation of two of these three explanations: (1) to demonstrate the importance of considering the age–sex distribution in death and in the population, and (2) to test the female frontline health workforce hypothesis among immigrants. The latter hypothesis stipulates that a high concentration of females (especially immigrants) working in the frontline health care and social assistance (HCSA) sector creates a condition for increased COVID-19 infection,Note 5, Note 10, Note 11 which may lead to subsequent death. A Statistics Canada study on COVID-19 deaths by immigrant status shows COVID‑19 crude death rates among immigrants to be higher than those among non-immigrants (26 and 22 per 100,000 population, respectively).Note 9 However, it is unknown whether there is a differential pattern of COVID-19 deaths by immigrant status by age and sex distribution in Canada. Since Quebec and Ontario were at first the hardest hit provinces by the pandemic, this study also presents overall results geographically.
The objectives of this study are to respond to the call by the PHAC report to monitor and explain the unique sex difference pattern in Canada and to ascertain whether the reported overrepresentation of female COVID-19 deaths in Canada persists over time.Note 8 This study also evaluates whether there is a sex difference in COVID-19 deaths by immigrant status in Canada and, if so, for which age groups and in which provinces or census metropolitan areas (CMAs). A secondary objective is to use the employer information from tax files of the deceased as a proxy to evaluate the female frontline health workforce hypothesis, using immigrants as a test case (corresponding non-immigrant death data linked to tax files are not presently available, though they are linkable).
Data and methods
Multiple key data sources were used in this study. First, following the PHAC report,8 updated data from the COVID-19 Sex-Disaggregated Data Tracker provided by Global Health 50/50 were used to examine the sex difference of COVID-19 deaths internationally.Note 12 Second, to examine the sex differential in COVID-19 deaths with immigration, a linkage of deaths from provisional data from the Canadian Vital Statistics - Death database (pCVSD) to the IMDB allowed for the comparison of COVID-19 deaths by immigrant status overall and for males and females separately.Note 13 In addition, the 2016 Census provides the denominator in the derivation of overall and age-specific death rates by immigrant status at various levels of geography for a proper comparison of COVID-19 mortality by sex in Canada.Note 14 All derivations using the linked dataset were based on rounded figures.
The COVID-19 Sex-Disaggregated Data Tracker data collection is coordinated by Global Health 50/50; the African Population and Health Research Center in Kenya; and the International Center for Research on Women, a global organization with offices in the United States, Asia, and Africa.Note 12 The tracker uses national data from all over the world (including Canada) to track COVID-19 infections and deaths, from the onset of the pandemic in 2020 onward. The male-to-female ratio of deaths related to COVID-19 was used as an indicator in the PHAC report, as derived by the quotient of the cumulative numbers of COVID-19 deaths of males over the corresponding numbers of females for a certain reporting country.Note 8 A value of 1 reflects parity, while a value higher than 1 denotes more males than females dying of COVID-19. Comparisons in this study were made at the baseline (June 2020 in Figure 1) and over time (to June 2021 in Figure 3) with Finland, a country reported to have a similar sex differential COVID-19 death pattern as Canada. Comparisons were also made with the United States and France, two highly affected countries reported by PHAC to have no confirmed reported COVID-19 death data by sex at the outset of the pandemic.Note 8 England, as a traditional immigration source for Canada, was also added for reference.
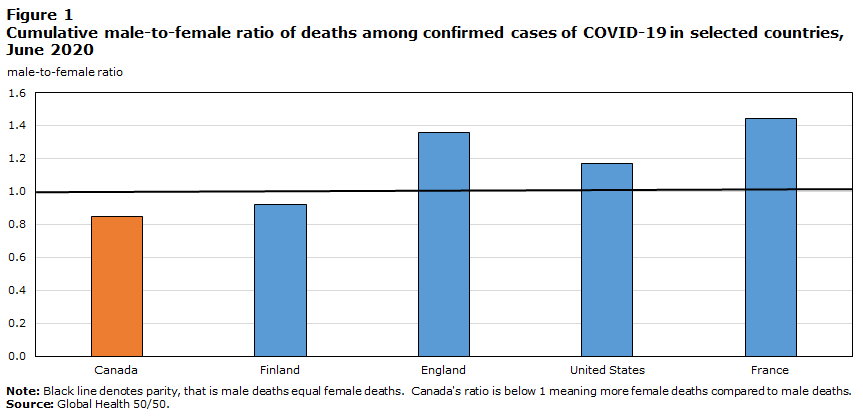
Description of Figure 1
| Canada | Finland | England | United States | France | |
|---|---|---|---|---|---|
| male-to-female ratio | |||||
| 0.85 | 0.92 | 1.36 | 1.17 | 1.44 | |
|
Note: Black line denotes parity, that is male deaths equal female deaths. Canada's ratio is below 1 meaning more female deaths compared to male deaths. Source: Global Health 50/50. |
|||||
Global Health 50/50 does not have data by immigrant status. This paper uses the 2020 provisional COVID-19 death data (from January to July 2020) linked to the 2018 IMDB to evaluate whether there is an inversion of the pattern of male-to-female COVID-19 death ratio by immigrant status (Figure 2).Note 13 The pCVSD captured all provisional death data from January 1 to July 4, 2020, provided to Statistics Canada by the provinces and territories except for Yukon. The dataset includes demographic information for people who died in these jurisdictions. The 2018 IMDB, which contains demographic and administrative information, such as age, sex, and country of birth, is an immigration database based on admission records for all immigrants since 1952 and non-permanent residents since 1980.Note 15 The linkage of provisional deaths in 2020 was conducted in Statistics Canada’s Social Data Linkage Environment, which linked the separate data sources to the Derived Record Depository, a national dynamic relational database at Statistics Canada that contains only basic personal identifiers to protect the confidentiality of individuals.Note 16 Through the IMDB–pCVSD linkage, data are available for COVID-19 deaths among IMDB immigrants. The remaining COVID-19 deaths (i.e., those that were not linked to the IMDB) are accounted for by the Canadian-born population and possibly a small number of immigrants who immigrated before 1952. For the purposes of this paper, these non-linked deaths will be described as deaths among non-immigrants.
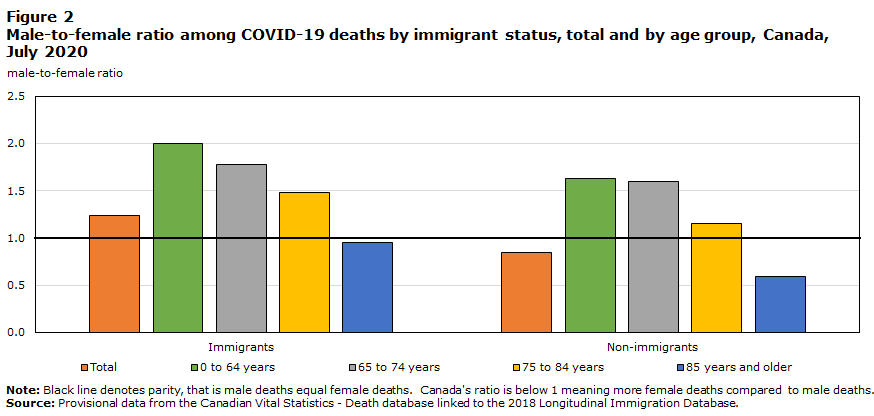
Description of Figure 2
| Immigrants | Non-immigrants | |
|---|---|---|
| male to female ratio | ||
| Total | 1.2 | 0.8 |
| 0 to 64 years | 2.0 | 1.6 |
| 65 to 74 years | 1.8 | 1.6 |
| 75 to 84 years | 1.5 | 1.2 |
| 85 years and older | 0.9 | 0.6 |
|
Note: Black line denotes parity, that is male deaths equal female deaths. Canada's ratio is below 1 meaning more female deaths compared to male deaths. Source: Provisional data from the Canadian Vital Statistics - Death database linked to the 2018 Longitudinal Immigration Database. |
||
Based on the IMDB–pCVSD linkage using death data up to July 2020, the male-to-female ratios of confirmed COVID‑19 deaths (Figure 2) and the relative death burden ratio attributable to COVID-19 accounted for by immigrants (Table 1) are derived to examine the differential patterns in COVID-19 deaths by immigrant status, by age group, by province, and in the three CMAs with the largest population of immigrants in Canada. The relative death burden ratio attributable to COVID-19 accounted for by immigrants is calculated as the ratio of the percentage of COVID-19 deaths occurring among IMDB immigrants arriving between 1952 and 2018 relative to their estimated population share, with the latter obtained from the 2016 Census.Note 14 A ratio greater than 1 means that the COVID-19 death burden of IMDB immigrants was disproportionately higher than their population share. The comparison is the distribution of deaths by immigrant status for males and females separately, which reveals the pattern of sex differences by immigrant status.Note 9 For the derivation of the age-sex specific death rates in Table 2, denominators were obtained from the 2016 Census by immigrant status for accurate comparisons of COVID-19 deaths.Note 14 Death certificates in Canada do not contain occupational information, but the immigration landing records of IMDB immigrants have been linked to administrative tax data since 1982. Employer information available from these tax data was used to evaluate the distribution of the immigrant frontline health workforce by sex. Through this linkage to tax information, the industrial affiliation was obtained through the employer information on the T4 supplemental tax files (Table 3). Code 62 in the North American Industry Classification System refers to the HCSA sector, which includes ambulatory health care services, hospitals, and nursing and residential care facilities.Note 15 This information was used to derive the proportion of deaths in workers from the HCSA sector and other major sectors by sex among immigrants.
| Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Immigrants (N=1,055) |
Non-immigrantsTable 1 Note 2 (N=2,680) |
Proportion of COVID-19 deaths accounted for by immigrants |
Proportion of immigrants according to the 2016 Census |
Relative death burden ratio accounted for by immigrantsTable 1 Note 1 |
Immigrants (N=855) |
Non-immigrantsTable 1 Note 2 (N=3,180) |
Proportion of COVID-19 deaths accounted for by immigrants |
Proportion of immigrants according to the 2016 Census |
Relative death burden ratio accounted for by immigrantsTable 1 Note 1 |
|
| Percent | Ratio | Percent | Ratio | |||||||
| Total | 100 | 100 | 28 | 21 | 1.3 | 100 | 100 | 21 | 23 | 0.9 |
| Age at death (years) | ||||||||||
| 0 to 64 | 9 | 7 | 32 | 20 | 1.6 | 5 | 4 | 27 | 21 | 1.3 |
| 65 to 74 | 15 | 15 | 28 | 27 | 1.0 | 11 | 8 | 26 | 28 | 0.9 |
| 75 to 84 | 32 | 32 | 28 | 32 | 0.9 | 27 | 24 | 23 | 31 | 0.8 |
| 85 and older | 44 | 45 | 28 | 31 | 0.9 | 57 | 64 | 19 | 28 | 0.7 |
| ProvinceTable 1 Note 3 | ||||||||||
| Quebec | 49 | 74 | 21 | 13 | 1.5 | 48 | 72 | 15 | 14 | 1.1 |
| Ontario | 44 | 21 | 44 | 28 | 1.6 | 47 | 23 | 36 | 30 | 1.2 |
| British Columbia | 4 | 2 | 47 | 27 | 1.7 | 3 | 2 | 33 | 30 | 1.1 |
| Census metropolitan areaTable 1 Note 3 | ||||||||||
| Montréal | 48 | 59 | 25 | 23 | 1.1 | 47 | 58 | 18 | 24 | 0.8 |
| Toronto | 35 | 10 | 57 | 45 | 1.3 | 39 | 12 | 46 | 48 | 0.9 |
| Vancouver | 4 | 1 | 50 | 40 | 1.3 | 3 | 1 | 38 | 44 | 0.9 |
|
||||||||||
| Overall | Immigrants | Non-immigrantsTable 2 Note 1 | ||||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| Total | 22.4 | 23.4 | 29.8 | 22.0Note * | 20.3 | 23.8Note * |
| Age at death (years) | ||||||
| 0 to 64 | 2.0 | 1.2Note * | 3.2 | 1.5Note * | 1.7 | 1.1Note * |
| 65 to 74 | 36.3 | 20.3Note * | 36.6 | 18.9Note * | 35.8 | 20.9Note * |
| 75 to 84 | 162.4 | 111.1Note * | 144.3 | 84.5Note * | 170.7 | 123.8Note * |
| 85 and older | 813.6 | 797.3 | 735.9 | 552.3Note * | 852.0 | 892.3 |
| ProvinceTable 2 Note 2 | ||||||
| Quebec | 63.7 | 65.3 | 97.9 | 73.7Note * | 58.5 | 66.8Note * |
| Ontario | 16.2 | 17.2 | 25.8 | 20.2Note * | 12.5 | 15.9Note * |
| British Columbia | 4.3 | 3.3 | 7.6 | 3.7Note * | 3.1 | 3.1 |
| Census metropolitan areaTable 2 Note 2 | ||||||
| Montréal | 107.8 | 111.0 | 113.5 | 83.4Note * | 106.1 | 119.6Note * |
| Toronto | 23.2 | 24.6 | 29.3 | 23.2Note * | 18.1 | 26.0Note * |
| Vancouver | 7.4 | 5.7 | 8.7 | 4.8 | 5.8 | 5.9 |
|
||||||
| Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|
| Proportion of COVID-19 deaths (N=95) |
Proportion of immigrants with T4 form in 2018 (N=2,385,600) |
COVID-19 death rate |
Proportion of COVID-19 deaths (N=30) |
Proportion of immigrants with T4 form in 2018 (N=2,181,400) |
COVID-19 death rate |
|||
| % | Per 100,000 population | Ranking | % | Per 100,000 population | Ranking | |||
| Employment sector | ||||||||
| Health care and social assistance (North American Industry Classification System [NAICS] 62) | 10 | 4 | 10.7 | 1 | 33 | 16 | 2.9 | 1 |
| Retail trade; professional, scientific and technical services (NAICS 44, 45, 54) | 20 | 18 | 4.6 | 4 | 17 | 18 | 1.3 | 2 |
| All others | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | 50 | 66 | 1.0 | 3 |
| Manufacturing (NAICS 31, 32, 33) | 20 | 15 | 5.3 | 2 | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable |
| Administrative and support, waste management and remediation services (NAICS 56) | 11 | 8 | 5.3 | 2 | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable |
| Transportation and warehousing (NAICS 48, 49) | 8 | 7 | 4.8 | 3 | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable |
| Other sectors | 31 | 49 | 2.6 | 5 | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable |
| Total | 100 | 100 | 4.0 | 100 | 100 | 1.4 | ||
|
... not applicable Source: Provisional data from the Canadian Vital Statistics - Death database linked to the 2018 Longitudinal Immigration Database. |
||||||||
Results
Revisiting the male-to-female ratio: An international comparison
Figure 1 shows that in the early months of the pandemic, both Canada and Finland had low male-to-female ratios of COVID-19 deaths (around 0.8), which indicate more female than male COVID-19 deaths in these countries.Note 9 By contrast, the United States, England, and France had higher male-to-female ratios of COVID-19 deaths, at 1.2, 1.4, and 1.4, respectively, suggesting that these countries had more male than female COVID-19 deaths at the outset of the pandemic.
Figure 2 shows the male-to-female COVID-19 death ratios for Canada by immigrant status, overall and by age group. The overall male-to-female ratios for immigrants and non-immigrants were 1.2 and 0.8, respectively. By age group, the ratio was higher than 1 from the youngest age group to the group aged 75 to 84 for both immigrants and non-immigrants. The higher proportion of females over males in COVID-19 deaths was observed only in the group aged 85 and older and was greater for non-immigrants (0.6) than for immigrants (0.9).
International trend lines of proportion of COVID-19 deaths by sex
Figure 3 shows that female overrepresentation in COVID-19 deaths was sustained from May 2020 until early 2021 in Canada. However, by the summer of 2021, the sex difference in COVID-19 deaths in Canada had reached parity. Finland had a similar trend, but reached parity before March 2021, earlier than in Canada. The United States, England, and France had persistently higher proportions of COVID-19 deaths among males compared with females, and England showed a 14% decline of the ratio from approximately 1.4 to 1.2.

Description of Figure 3
| Time (month by year) | Canada | Finland | England | United States | France |
|---|---|---|---|---|---|
| male to female ratio | |||||
| 2020 | |||||
| June | 0.9 | 0.9 | 1.4 | 1.2 | 1.4 |
| September | 0.8 | 0.9 | 1.3 | 1.2 | 1.4 |
| December | 0.9 | 1.0 | 1.3 | 1.2 | 1.4 |
| 2021 | |||||
| March | 1.0 | 1.0 | 1.2 | 1.2 | 1.4 |
| June | 1.0 | 1.1 | 1.2 | 1.2 | 1.4 |
|
Note: Black line denotes parity, that is male deaths equal female deaths. Canada's ratio is below 1 meaning more female deaths compared to male deaths. Source: Global Health 50/50. |
|||||
Distribution and proportion of deaths attributable to COVID-19 by sex and immigrant status
Table 1 corroborated results from Figure 2 to show that the higher proportion of female over male COVID-19 deaths was evident only among non-immigrants. Among females, immigrants accounted for 21% of COVID-19 deaths but 23% of the total female population in Canada, yielding a relative death burden ratio of 0.9 (i.e., underrepresentation of immigrants among female COVID-19 deaths). Among the male population, immigrants accounted for 28% of COVID-19 deaths, but represented 21% of the total male population in Canada, yielding a relative death burden ratio of 1.3 (i.e., an overrepresentation of immigrants among male COVID-19 deaths). Furthermore, the overrepresentation of immigrants among male deaths attributable to COVID-19 was especially concentrated in the population aged younger than 65. Among males, immigrants represented 20% of the total population aged younger than 65, but represented 32% of COVID-19 deaths (a relative death burden ratio of 1.6) compared with 27% among females in this age group. Variations in the distribution of COVID-19 deaths by province and CMA for males and females were also observed. For example, in Montréal, immigrants accounted for 24% of the total female population but 18% of COVID-19 deaths among females, whereas in Toronto, immigrants accounted for 48% of the total female population and 46% of COVID-19 deaths among females. The proportions of COVID-19 deaths among immigrant males in Montréal and Toronto were higher (25% and 57%, respectively).
From death counts to death rates
Table 2 shows that, for COVID-19 deaths up to July 2020, while the overall death rate in Canada was slightly higher for females than for males, the difference was not statistically significant. Analysis by age group shows significantly higher COVID‑19 death rates for males than for females in all age groups for the total population, except for those aged 85 and older, where the sex difference in the COVID-19 death rate was not statistically significant.
By immigrant status, however, there was a higher COVID-19 death rate for females over males among non-immigrants and a higher COVID-19 death rate for males over females among immigrants. Age-specific death rates were higher for males than for females in all age groups regardless of immigrant status, except for those aged 85 and older among non-immigrants. Geographically, while a higher female COVID-19 death rate was observed only among the non-immigrant populations in Quebec and Ontario, in particular in Montréal and Toronto, the results were reversed for immigrant populations with higher male death rates.
Frontline female immigrant health care workers and COVID-19 deaths
Table 3 shows the distribution of COVID-19 deaths by industry of employment and sex among immigrants who filed taxes in 2017 that included industry affiliation information. Since the majority of COVID-19 deaths at the onset of the pandemic were concentrated among seniors (i.e., those aged 65 and older), the linked dataset contains only 125 deaths among immigrants, whose tax records have an associated industry code on file to help determine their employment industry information. The present analysis shows that the number of deaths from the IMDB tax filers with industrial affiliation information was small, with only around 95 male deaths and 30 female deaths—too few to draw conclusive evidence.
The distribution of industry of employment by sex among immigrant tax filers shows that 4% of the 2.3 million immigrant males who filed taxes in 2017 (or approximately 85,000 male immigrants) worked in the HCSA sector, compared with 16% of the nearly 2.2 million immigrant female tax filers (or approximately 350,000 female immigrants). Thus, immigrant females were highly concentrated in the HCSA sector. However, the COVID-19 death rate among HCSA immigrant workers was higher among males compared with females (10.7 vs. 2.9 per 100,000 population).
Discussion
The purpose of this paper is to investigate why Canada is an anomaly in the global phenomenon of male overrepresentation in COVID-19 deaths during the onset of the pandemic in 2020. The results showed that the higher proportion of females among COVID-19 deaths initially observed in Canada in early 2020 eventually evened out in the summer of 2021, when the male-to-female death ratio reached parity. The decline of the overrepresentation of females among COVID-19 deaths may be attributable to early-2021 COVID-19 vaccination efforts in Canada among the oldest age groups, which are more heavily skewed towards females.Note 17 The Canadian Institute for Health Information reported that up to 81% of COVID-19 deaths in the early period of the pandemic occurred in long-term care facilities, compared with an average of 38% in other Organisation for Economic Co-operation and Development countries (ranging from less than 10% in Slovenia and Hungary to 66% in Spain).Note 18 The present study indicates that more than 50% of COVID-19 deaths occurred among those aged 85 and older (54.1%). As such, it is highly plausible that the initial overrepresentation of females among COVID‑19 deaths was related to the fact that two out of three long-term care facility residents are female.Note 6 By early 2021, long-term care facility residents and staff were prioritized to receive COVID‑19 vaccinations. By the end of March 2021, 95% of long-term care facility residents had received their first dose of the vaccine, compared with 3% of the general public. The high vaccination rate among long-term care facility residents reduced both infections and the severity of COVID-19 outcomes—including deaths—among this group by over 90%.Note 17 At the provincial level, similar to the national level, the results show that the higher proportion of female deaths attributable to COVID-19 was observed only among the non-immigrant population in Quebec and Ontario, in particular Montréal and Toronto, where a sizable number of COVID-19 deaths were attributable to those living in long-term care facilities with higher proportions of female residents.Note 17 By contrast, a study of excess deaths in long-term care facilities in Ontario revealed that, even in the long-term care context, the 30-day mortality rate among females who tested positive for COVID-19 was still statistically lower than that of their male counterparts (hazard rate of 0.58).Note 19 This finding may indicate that if testing and infection information is available at the individual level, higher male COVID-19 mortality may still be observed even within the context of the long-term care facility. For immigrant status, a first look at COVID-19 mortality by nativity in Minnesota also mirrored the current findings; for the foreign-born population like the Latino immigrant population, COVID-19 deaths were concentrated in relatively younger and working-age men, while for the majority of the U.S.-born population, COVID-19 deaths were concentrated in long-term care facilities.Note 20
The present study provides further support on the role of the age and sex distribution of the affected population and the immigrant status to reconcile the initial observed female overrepresentation in COVID-19 deaths. Because of the differential life expectancy by sex, with longer life expectancy of females compared with males, the results of the study are not surprising. If the deaths are disproportionately happening in the oldest age group (i.e., those aged 85 and older), examining the proportion of deaths by sex is expected to result in more female deaths, everything else held constant.Note 21, Note 22 During the onset of the pandemic, approximately 50% of deaths occurred among those aged 85 and older. When considering the age–sex differential in population distribution by immigrant status, there was indeed a higher death rate for females among non-immigrants, compared with that among immigrants. The higher COVID-19 death rate among non-immigrants for those aged 85 and older is likely related to the fact that fewer immigrant females aged 85 and older were institutionalized compared with non-immigrant females.Note 23 The findings also show a higher death rate among immigrant males, compared with their female counterparts, possibly reflecting the biological and situational factors hypothesized in the literature for higher morbidity and mortality in males compared with females worldwide.
Regarding the hypothesis that posits that a high concentration of females (especially female immigrants) working in the frontline HCSA sector was at risk for increased COVID-19 infection, the current findings show that while there were more female than male immigrants working in HCSA, the HCSA-specific COVID-19 death rate was lower among female immigrants than among male immigrants. This finding may help to explain in part that the overrepresentation of male deaths attributable to COVID-19 among the immigrant population was especially concentrated in the population younger than 65; among males, immigrants represented 20% of the total population younger than 65, but 32% of COVID-19 deaths. The current industry-specific results for immigrants are based on small numbers since more than 95% of the COVID-19 deaths happened among those aged 65 and older, a group made up mostly of retirees and therefore with no employer (tax-linked) information. As well, corresponding results for non-immigrants would be informative, but their COVID-19 death records were not linked to tax records at the time of this analysis. Future analyses with linkages between all COVID-19 deaths and tax files, as well as additional deaths for more months of observations, could provide the platform for a more in-depth examination. It could shed light on sex differences in COVID-19 mortality by industry between immigrants and non-immigrants.
Two limitations should be noted for this study. First, the COVID-19 deaths analyzed are from provisional death data that make up a preliminary dataset that does not cover 100% of deaths in the reference period. Coverage may vary by jurisdiction based on various factors, including collection methods, and death counts are subject to change because of the provisional nature of the data.Note 9, Note 14 Second, 2016 Census data used to derive death rates attributable to COVID-19 in 2020 were the best proxy available, but the age- and sex-specific population size may have changed over the lapsed years. Future analyses could use 2021 Census data as the denominator to validate the rate derivation.
Given the impact of initial COVID-19 infection on those who are at the lower end of the spectrum of the social determinants of health, other factors like socioeconomic status or race, which tend to cut across multiple sectors, could be at play to result in increased immigrant death rates. Future study with the required data could evaluate that possibility. As well, differences in age distribution between males and females may have contributed to Canada’s overrepresentation of COVID-19-related female deaths, which contrasts with many other countries. Estimating age-standardized death rates by sex could provide another perspective on the differences between Canadian findings and those of other countries. Also, this study used a linkage between death data and the IMDB, but a future study could expand the linkage to include the T1 tax files of non-immigrants and immigrants who landed before 1952, which were not included in the IMDB. Such research could provide a more complete understanding of the gender differences in COVID-19 deaths between immigrants and non-immigrants.
In summary, this study provides initial insights into the sex differences in COVID-19 deaths in Canada by immigrant status and shows an overrepresentation of male COVID-19 deaths among the immigrant population. Future monitoring, research, and data development are needed to shed light on the differential pathways by sex from exposure to COVID-19 infection and possible death through which the sex differences in COVID-19 mortality emerge.
Acknowledgment
The author gratefully acknowledges funding from the Women and Gender Equality Canada (WAGE) for project support.
- Date modified: