
Health Reports
Correlates of vaping among adolescents in Canada

DOI: https://www.doi.org/10.25318/82-003-x202200700003-eng
Abstract
Background
Vaping is more prevalent among younger than older Canadians. While vaping is less harmful than combustible tobacco, it is not without health risk.
Data and methods
Data from the 2019 Canadian Health Survey on Children and Youth were used to estimate vaping prevalence. Logistic regression models assessed the association of sociodemographic, youth, parenting and peer factors with vaping. The 2020 Canadian Community Health Survey identified adolescents who reported vaping before tobacco smoking. Data from the 2019 Canadian Tobacco and Nicotine Survey were used to examine vaping of e-liquids containing nicotine and flavours.
Results
Vaping rates for 15- to 17-year-olds were nearly four times (21.3%) higher than those of 12- to 14-year-olds (5.4%). Two-thirds (66.1%) of 12- to 17-year-olds who had used both tobacco and e-cigarettes reported trying e-cigarettes first. E-liquids containing nicotine were used by 89.3% of 15- to 19-year-olds who reported vaping in the past 30 days; comparable with older adults. For both younger and older adolescents, having friends who engaged in negative behaviours, having been employed, and having consumed alcohol increased the odds. For 12- to 14-year-olds, attention deficit hyperactivity disorder was a risk factor, whereas having parents who usually knew who they were with and higher relatedness scores were protective. Among older adolescents, being male, being Canadian-born, having lower grades, and using tobacco or cannabis increased the odds of vaping.
Interpretation
An adolescent’s risk of vaping was most strongly correlated with other substance use, although other youth, parenting and peer characteristics also mattered. Because most of the data presented were collected before the COVID-19 pandemic and new vaping regulations, ongoing monitoring remains important.
Keywords
E-cigarettes, cross-sectional study, tobacco alternatives, risk factors, nicotine or flavour-based vaping
Authors
Michelle Rotermann (michelle.rotermann@statcan.gc.ca) and Heather Gilmour are with the Health Analysis Division, Analytical Studies and Modelling Branch, Statistics Canada, Ottawa.
What is already known on this subject?
- While vaping may be less harmful than inhalation of regular tobacco smoke, it is not without health risks nor is it considered safe for individuals who are not already consumers of tobacco products.
- Vaping rates have been increasing since e-cigarettes were introduced to North America, with rates tending to be higher among adolescents, raising concerns about nicotine dependence and impacts on tobacco cigarette smoking rates.
- Less is known about the influence of peers (friends) and parents on an adolescent’s risk of vaping, as monitoring surveys typically do not include this information.
What does this study add?
- Few nationally representative Canadian studies of vaping include adolescents as young as 12 years of age.
- Rates of vaping among adolescents aged 15 to 17 years were nearly four times (21.3%) higher than those of 12- to 14-year-olds (5.4%). Among 15- to 17-year-olds, 5.3% both vaped and used tobacco products.
- About 9 in 10 (89.3%) adolescents aged 15 to 19 years of age who reported vaping in the past 30 days reported using e-liquids containing nicotine; comparable with the estimates for older Canadians.
- Having friends who engaged in negative behaviours, being employed, and alcohol consumption increased the odds of vaping for both younger (aged 12 to 14) and older (aged 15 to 17) adolescents. Additionally, 12- to 14-year-olds with attention deficit hyperactivity disorder were at increased risk of vaping, whereas adolescents who reported that their parents usually knew who they were with and those reporting higher relatedness scores had a lower risk. Being male, Canadian-born, having lower grades, and using tobacco or cannabis were other vaping risk factors for older adolescents.
Introduction
Vaping is the act of inhaling and exhaling vapour, which can include nicotine and flavourings, produced by devices such as electronic cigarettes (e-cigarettes), vape pens, vape mods, or vaporizers. Recent devices are rechargeable, can resemble compact USB flash drives, and often use nicotine salts, which tend to contain more nicotine than liquids.Note 1 Nicotine is a highly addictive substance that affects attention, cognition and mood and can affect developing adolescent brains.Note 2Note 3
E-cigarettes and related devices have been promoted as less harmful than tobacco cigarettes and as smoking-cessation (or reduction) aids. While vaping may be less harmful than the inhalation of smoke from tobacco, it poses risks of nicotine dependence, other substance use, and respiratory and cardiovascular disease.Note 4Note 5 The 2019/2020 outbreak of e-cigarette or vaping use-associated lung injury (EVALI), for example, hospitalized several thousand and killed dozens in the United States.Note 6 A similar vaping-associated lung illness (VALI) outbreak was investigated in Canada.Note 7 There are also concerns that vaping may increase the risk of contracting COVID-19, although evidence is inconclusive.Note 8Note 9Note 10
Vaping has been increasing in Canada since monitoring began,Note 11Note 12Note 13 and is more common among 15- to 24-year-olds than older people.Note 14 It is feared that the widespread adoption of vaping may undermine longer-term reductions in smoking and lead to the re-normalization of tobacco use.Note 4 More Canadian students report having tried e-cigarettes than tobacco cigarettes in their lifetime,Note 15 and growing numbers of vapers have never been cigarette smokers.Note 16Note 17Note 18 Some longitudinal research also finds that vapers are more likely to start cigarette smoking than non-vapers.Note 19Note 20
An understanding of the factors that put younger and older adolescents at higher risk of vaping, and an understanding of protective factors are important and policy-relevant. Previous analyses have been limited by few covariates and lack of representativeness, and have examined older adolescents, primarily using US data, which may not generalize to the Canadian situation.Note 1Note 21Note 22Note 23Note 24 The use of three complementary data sources helps to present a more complete picture of vaping by adolescents in Canada.
The primary objective of this study is to examine vaping in the past 30 days among 12- to 17-year-olds stratified by age, 12- to 14-year-olds and 15- to 17-year-olds, in addition to other correlates, using 2019 Canadian Health Survey on Children and Youth (CHSCY) data. The secondary objectives were to identify adolescents who reported vaping before tobacco smoking and to examine the vaping of nicotine and flavoured e-liquids using data from the 2020 Canadian Community Health Survey (CCHS) and the 2019 Canadian Tobacco and Nicotine Survey (CTNS).
Methods
Data sources
The cross-sectional 2019 CHSCY collected detailed data on health status, care utilization, behaviours and determinants of children and youth in Canada.Note 25 Data were collected using an electronic questionnaire, primarily self-completed, although interviewer assistance via the telephone was also available. Collection took place between February and August 2019 and covered the population aged 1 to 17, as of January 31, 2019, living in the 10 provinces and the 3 territories.
The initial questionnaire was administered to the person most knowledgeable about the selected young person; the second was administered directly to the selected respondent aged 12 to 17 and asked about behaviours including cigarette smoking, vaping and drinking. The overall CHSCY response rate was 52.1%, while that for youth aged 12 to 17 years was 41.3% (13,602 respondents; 6,687 aged 12 to 14 years; 6,915 aged 15 to 17 years).
The cross-sectional Canadian Community Health Survey (CCHS) 2020 covers the population aged 12 and older.Note 26 Health Canada sponsored a rapid response (RR) module on smoking stages of change, tobacco alternatives and vaping which was collected in the provinces from a sample of 31,417 overall, corresponding to a 29.3% response rate. The sample included 2,495 respondents aged 12 to 17 years.
Excluded from the CHSCY and CCHS RR module’s survey coverage were children and youth living on First Nations reserves and other Aboriginal settlements in the provinces, in foster homes (CHSCY), in foster care (CCHS), or in institutions. Persons living in the Quebec health regions of Région du Nunavik and Région des Terres-Cries-de-la-Baie-James were also excluded from the CCHS. The CHSCY covers approximately 98% of the Canadian population aged 1 to 17 in all provinces and 96% in the territories. The CCHS covers about 97% of the Canadian population aged 12 and older.
The cross-sectional 2019 Canadian Tobacco and Nicotine Survey (CTNS) covers the non-institutionalized population 15 years of age and older across all 10 provinces who are not living on First Nations reserves and other Aboriginal settlements.Note 27 Data were collected from October to December 2019 using an electronic questionnaire and telephone follow-up from 8,614 respondents, corresponding to a 44.4% response rate. The CTNS covers approximately 95% of the Canadian population aged 15 and older.
Definitions
Vaping and tobacco use
Adolescents aged 12 to 17 years were asked by the CHSCY whether they had used an e-cigarette (vaporizer with e-juice, vape pen, tank, mod) in the past 30 days, as well as how often (less than once per week, one to two times per week, three to five times per week, daily or almost every day).
Use of tobacco products (cigarettes, cigars, little cigars or cigarillos, or a water pipe) was ascertained from other CHSCY questions about the frequency of use in the past 30 days. Individuals who used at least one product were grouped and compared with those reporting no use.
Four e-cigarette and tobacco product use categories were created from the tobacco, e-cigarette and other tobacco product CHSCY questions: e-cigarette only, e-cigarette and tobacco product(s), tobacco product(s) but not e-cigarettes, none.
On the CCHS RR module, those who had smoked both cigarettes (currently a daily or occasional smoker or have smoked a whole cigarette in their lifetime) and vaped were asked, “Which did you try first, an e-cigarette / vaping device or a cigarette?”
CTNS respondents who reported vaping in the past 30 days were asked about the products they used. For example, “On how many days did you vape an e-liquid, with or without nicotine?” Those who reported at least one day of vaping with nicotine, were considered to have vaped an e-liquid containing nicotine. Because individuals could report more than one e-liquid, estimates do not add to 100%. E-liquids can also be flavoured, and respondents were asked which flavour they used most often. The questionnaire asked about 10 different flavours that were collapsed into 4 categories: tobacco; fruit, candy or dessert; mint or menthol; other (coffee or tea, alcohol, flavourless, no usual flavour and other).
Covariates
Selection of covariates for the multivariable analyses was guided by the literature and data availability in the CHSCY and included sociodemographic, youth, parenting and peer characteristics.
Two age groups (12 to 14 years compared with 15 to 17 years) were used to stratify the 30-day vaping analyses.
Sex at birth was coded as male or female. Family structure describing the living arrangements of the adolescent was categorized as living with two biological parents or not. Respondents were categorized as Canadian- or foreign-born (including landed and non-permanent residents). Because of sample size constraints, Indigenous identity was dichotomized as Indigenous (including First Nations, Métis or Inuk [Inuit]) and non-Indigenous. Household income was categorized as below $40,000, $40,000 to less than $100,000, or $100,000 or more. Two dichotomous variables for having been diagnosed with a mood or anxiety disorder and attention deficit hyperactivity disorder (ADHD) were also included.
Whether the adolescent had used cigarettes or smoked tobacco in the previous 30 days, or had used cannabis at least monthly versus less frequently (or not at all) in the previous 3 months was assessed. Past-year alcohol use compared regular or occasional drinkers with those who did not report drinking.
The Children’s Intrinsic Needs Satisfaction Scale (CINSS) correlates with emotional well-being using three subscales: relatedness, competence and autonomy.Note 28Note 29Note 30 Relatedness involves a sense of closeness and belonging; competence involves a sense of self-efficacy or mastery; and autonomy involves a perception of choice and control over activities. For bivariate analyses, subscale scores were dichotomized (median or above versus below) and left continuous in multivariable analyses.
Those who were paid by an employer or for odd jobs, or worked on their family’s farm or business were considered to have been employed in the past 12 months. Having a family member who smoked (including cigarettes, cigars or pipe tobacco) was coded as yes or no. School performance was based on the self-reported approximate overall mark this year: mainly As compared with lower marks (including those not in school).
Indicators of the strength of the parent–adolescent relationship included whether “parents usually knew who you were with when you were away from home,” either frequently (often or most of the time) or infrequently (sometimes, rarely or never), and how often the adolescent “spent time just talking with parents,” either frequently (daily or weekly) or infrequently (monthly, a few times a year, never).
Adolescents were asked about how many of their close friends (all, most, some or none) engaged in or endorsed the following four behaviours: think it is okay to work hard at school (reverse coded), cut or skipped a day of school without permission, drink alcohol, or have a reputation for causing trouble. A composite variable was created to indicate that the adolescent thought that at least one of the four behaviours described most or all of their friends.
Analytical techniques
Weighted frequencies and cross-tabulations were calculated to examine estimates of vaping by selected correlates and stratified by age. Multivariable logistic regression was used to determine factors independently associated with vaping after accounting for sociodemographic, youth, parenting and peer characteristics. Cigarettes or other tobacco use in the past 30 days and cannabis use in the past 3 months were omitted from the logistic regression for 12- to 14-year-olds because of the small number of respondents in this age group that engaged in these behaviours, causing model instability. Bootstrap weights were applied to account for underestimation of standard errors resulting from the complex survey design.Note 31 Analyses were performed using SAS 9.4 and SUDAAN 11.0.3.
Results
Prevalence of vaping
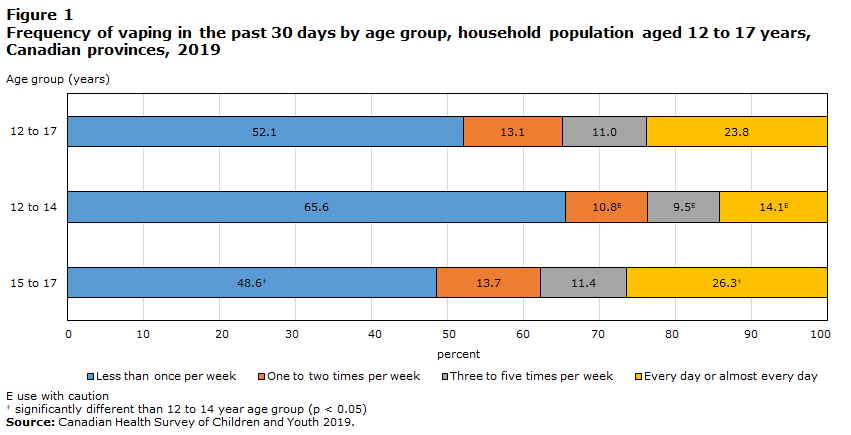
According to the 2019 CHSCY, 13.2% (95% confidence interval[CI]: 12.5% to 14.0%) of adolescents (nearly 300,000) aged 12 to 17 years reported vaping in the previous 30 days. Among them, nearly one-quarter (23.8%) did so daily or almost daily (Figure 1). For adolescents aged 15 to 17, rates were almost four times (21.3%) higher than for those aged 12 to 14 (5.4%) (Table 1). Older adolescents were also more likely to have used an e-cigarette daily or almost daily (26.3%) than younger adolescents (14.1%) (Figure 1).
Description for Figure 1
| Type of tobacco user by age group | |||
|---|---|---|---|
| 15 to 17 | 12 to 14 | 12 to 17 | |
| percent | |||
| Less than once per week | 48.6Data table for Figure 1 Note ‡ | 65.6 | 52.1 |
| One to two times per week | 13.7 | 10.8Note E: Use with caution | 13.1 |
| Three to five times per week | 11.4 | 9.5Note E: Use with caution | 11.0 |
| Every day or almost every day | 26.3Data table for Figure 1 Note ‡ | 14.1Note E: Use with caution | 23.8 |
E use with caution
|
|||
| Characteristics | 12 to 14 years | 15 to 17 years | ||||||
|---|---|---|---|---|---|---|---|---|
| '000s | % | 95% confidence interval |
'000s | % | 95% confidence interval |
|||
| from | to | from | to | |||||
| Total | 63.1 | 5.4 | 4.7 | 6.3 | 236.6 | 21.3 | 20.0 | 22.6 |
| Sociodemographic | ||||||||
| Sex | ||||||||
| Male | 34.2 | 5.7 | 4.7 | 6.9 | 132.8 | 23.4Table 1 Note ‡ | 21.6 | 25.4 |
| FemaleTable 1 Note † | 29.0 | 5.1 | 4.2 | 6.3 | 103.8 | 19.0 | 17.3 | 21.0 |
| Family structure (child lives with) | ||||||||
| Two biological parents | 35.8 | 4.4 | 3.7 | 5.2 | 139.6 | 19.5Table 1 Note ‡ | 18.0 | 21.0 |
| OtherTable 1 Note † | 27.2 | 8.2 | 6.6 | 10.3 | 93.9 | 24.6 | 22.2 | 27.1 |
| Canadian-born | ||||||||
| Yes | 60.1 | 6.1 | 5.3 | 7.0 | 218.6 | 24.3Table 1 Note ‡ | 22.8 | 25.8 |
| No, foreign-born (including landed and non-permanent residents)Table 1 Note † | 2.9 | Note F: too unreliable to be published | Note ...: not applicable | Note ...: not applicable | 16.4 | 7.9 | 6.2 | 10.0 |
| Indigenous identity | ||||||||
| Indigenous | 4.1Note E: Use with caution | 7.2Note E: Use with caution | 4.6 | 11.1 | 16.0 | 31.4Table 1 Note ‡ | 25.7 | 37.7 |
| Non-IndigenousTable 1 Note † | 59.0 | 5.4 | 4.6 | 6.2 | 218.3 | 20.7 | 19.4 | 22.0 |
| Household income | ||||||||
| Less than $40,000Table 1 Note † | 10.4Note E: Use with caution | 5.5Note E: Use with caution | 3.9 | 7.8 | 32.6 | 18.2 | 15.3 | 21.5 |
| $40,000 to less than $100,000 | 19.0 | 4.5 | 3.5 | 5.7 | 81.3 | 19.8 | 17.7 | 22.0 |
| $100,000 or more | 33.7 | 6.2 | 5.1 | 7.4 | 122.7 | 23.6Table 1 Note ‡ | 21.7 | 25.6 |
| Youth, parenting and peer | ||||||||
| Mood or anxiety disorder | ||||||||
| Yes | 7.3Note E: Use with caution | 10.5Note E: Use with caution Table 1 Note ‡ | 7.2 | 15.0 | 39.2 | 31.4Table 1 Note ‡ | 27.2 | 35.9 |
| NoTable 1 Note † | 55.8 | 5.1 | 4.4 | 6.0 | 197.3 | 20.0 | 18.7 | 21.4 |
| Attention deficit hyperactivity disorder | ||||||||
| Yes | 13.9Note E: Use with caution | 12.6Note E: Use with caution Table 1 Note ‡ | 9.0 | 17.4 | 39.7 | 34.2Table 1 Note ‡ | 29.0 | 39.7 |
| NoTable 1 Note † | 49.2 | 4.7 | 4.0 | 5.5 | 196.8 | 19.8 | 18.5 | 21.1 |
| Worked in the past 12 months | ||||||||
| Yes | 38.1 | 8.1 | 6.8 | 9.6 | 193.8 | 26.7Table 1 Note ‡ | 25.1 | 28.5 |
| NoTable 1 Note † | 25.1 | 3.7 | 2.9 | 4.6 | 41.5 | 10.8 | 9.3 | 12.6 |
| Overall mark in school | ||||||||
| Mainly ATable 1 Note † | 23.5 | 3.7 | 2.9 | 4.6 | 85.8 | 15.4 | 13.9 | 17.1 |
| Lower than A | 39.0 | 7.7 | 6.4 | 9.1 | 149.3 | 27.3Table 1 Note ‡ | 25.3 | 29.4 |
| Children's intrinsic needs satisfaction scale | ||||||||
| Relatedness | ||||||||
| Median (3.5) or above | 23.8 | 3.1 | 2.4 | 4.0 | 108.2 | 17.8Table 1 Note ‡ | 16.2 | 19.5 |
| Below medianTable 1 Note † | 39.3 | 10.0 | 8.5 | 11.8 | 128.3 | 25.5 | 23.5 | 27.5 |
| Competence | ||||||||
| Median (3.5) or above | 25.0 | 3.6 | 2.8 | 4.6 | 92.3 | 17.1Table 1 Note ‡ | 15.5 | 18.9 |
| Below medianTable 1 Note † | 38.1 | 8.1 | 6.9 | 9.6 | 144.2 | 25.2 | 23.3 | 27.1 |
| Autonomy | ||||||||
| Median (3.3) or above | 30.8 | 4.2 | 3.4 | 5.2 | 127.7 | 19.7Table 1 Note ‡ | 18.0 | 21.4 |
| Below medianTable 1 Note † | 32.3 | 7.6 | 6.3 | 9.1 | 108.8 | 23.6 | 21.6 | 25.7 |
| Alcohol use (past 12 months) | ||||||||
| Regular or occasional use | 35.2 | 34.8 | 29.4 | 40.7 | 202.4 | 42.8Table 1 Note ‡ | 40.4 | 45.3 |
| Not in the past 12 months or never had a drinkTable 1 Note † | 27.9 | 2.6 | 2.1 | 3.3 | 32.5 | 5.1 | 4.3 | 6.1 |
| Cigarettes or other tobacco use (past 30 days) | ||||||||
| Yes | 9.7Note E: Use with caution | 79.0 | 63.9 | 88.9 | 58.8 | 78.4Table 1 Note ‡ | 72.3 | 83.5 |
| NoTable 1 Note † | 53.4 | 4.7 | 4.0 | 5.4 | 176.5 | 17.1 | 15.9 | 18.3 |
| Cannabis use (past three months) | ||||||||
| At least monthly | 6.9Note E: Use with caution | 85.9 | 66.9 | 94.9 | 58.1 | 74.2Table 1 Note ‡ | 68.1 | 79.4 |
| Once or twice, or neverTable 1 Note † | 54.6 | 4.8 | 4.1 | 5.6 | 158.9 | 16.0 | 14.8 | 17.3 |
| Parents knew who child was with outside home | ||||||||
| Frequently | 45.3 | 4.3 | 3.7 | 5.1 | 194.4 | 20.0Table 1 Note ‡ | 18.7 | 21.4 |
| Infrequently or not at allTable 1 Note † | 17.6Note E: Use with caution | 16.4 | 12.5 | 21.3 | 40.0 | 29.6 | 25.7 | 33.9 |
| Spends time just talking with parents | ||||||||
| Frequently | 51.4 | 5.0 | 4.2 | 5.8 | 195.1 | 20.8 | 19.4 | 22.3 |
| Infrequently or not at allTable 1 Note † | 11.3Note E: Use with caution | 9.4Note E: Use with caution | 6.9 | 12.7 | 39.4 | 23.4 | 20.1 | 27.0 |
| Family member smokes (cigarettes, cigars or pipe tobacco) | ||||||||
| Yes | 20.8 | 8.2 | 6.5 | 10.3 | 80.7 | 31.1Table 1 Note ‡ | 28.2 | 34.3 |
| NoTable 1 Note † | 42.4 | 4.7 | 3.9 | 5.6 | 155.8 | 18.3 | 16.9 | 19.8 |
| Number of friends engaged in selected behaviours | ||||||||
| Most or all | 32.7 | 11.7 | 9.7 | 13.9 | 183.6 | 35.5Table 1 Note ‡ | 33.3 | 37.8 |
| None or someTable 1 Note † | 29.2 | 3.4 | 2.7 | 4.2 | 51.8 | 8.8 | 7.6 | 10.2 |
|
... not applicable E use with caution F too unreliable to be published
|
||||||||
The use of e-cigarettes and related vaping devices was not always the only tobacco product used. An estimated 5.3% of 15- to 17-year-olds and 0.8% of 12- to 14-year-olds reported using e-cigarettes and a tobacco product in the past 30 days (Table 2). However, the most prevalent group were those who used e-cigarettes exclusively (15.9% of 15- to 17-year-olds and 4.6% of 12- to 14-year-olds). The exclusive use of tobacco products was rare at 1.5% among 15- to 17-year-olds, and unreleasable for those aged 12 to 14 years.
| E-cigarette or tobacco product(s) use | 12 to 14 years | 15 to 17 years | ||||
|---|---|---|---|---|---|---|
| % | 95% confidence interval |
% | 95% confidence interval |
|||
| from | to | from | to | |||
| E-cigarette only | 4.6 | 4.0 | 5.4 | 15.9Table 2 Note ‡ | 14.8 | 17.1 |
| E-cigarette and tobacco product(s) | 0.8Note E: Use with caution | 0.6 | 1.2 | 5.3Table 2 Note ‡ | 4.6 | 6.1 |
| Tobacco product(s) but not e-cigarettes | Note F: too unreliable to be published | Note ...: not applicable | Note ...: not applicable | 1.5 | 1.1 | 1.9 |
| None | 94.3 | 93.5 | 95.1 | 77.3Table 2 Note ‡ | 76.0 | 78.6 |
|
... not applicable E use with caution F too unreliable to be published
|
||||||
Vaping preceded the smoking of tobacco cigarettes
Analysis of the 2020 CCHS data of 12- to 17-year-olds who reported having used both electronic and tobacco cigarettes estimated that, for two-thirds (66.1%; 95% CI: 54.2% to 76.2%), e-cigarette use preceded smoking of tobacco cigarettes (Data not shown in table). Comparatively, this was the case for one-third of 18- to 24-year-olds (33.4%; 95% CI: 26.9% to 40.7%).
E-liquids containing nicotine were used by the majority, regardless of age
According to the 2019 CTNS, about 9 in 10 (89.3%) 15- to 19-year-olds who reported vaping in the past 30 days reported using e-liquids containing nicotine, comparable with the estimates for older vapers (Table 3). By contrast, fruit-, candy- and dessert-flavoured vape products were more commonly used by youth aged 15 to 19 than adults aged 25 or older (61.6% compared with 42.7%).
| Among those who vaped in the past 30 days | 15 to 19 yearsTable 3 Note † | 20 to 24 years | 25 or older | ||||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% confidence interval |
% | 95% confidence interval |
% | 95% confidence interval |
||||
| from | to | from | to | from | to | ||||
| Used e-liquid containingTable 3 Note ‡ | |||||||||
| Nicotine | 89.3 | 83.2 | 93.4 | 86.5 | 79.6 | 91.3 | 80.6 | 71.8 | 87.2 |
| No nicotine | 23.7 | 17.4 | 31.5 | 17.6Note E: Use with caution | 11.8 | 25.4 | 16.5Note E: Use with caution | 10.3 | 25.5 |
| Most often used flavour | |||||||||
| Fruit, candy or dessert | 61.6 | 53.6 | 69.0 | 57.1 | 47.8 | 66.0 | 42.7 Note * | 33.5 | 52.4 |
| Mint or menthol | 17.4Note E: Use with caution | 12.1 | 24.3 | 24.8 | 17.9 | 33.3 | 15.3Note E: Use with caution | 9.5 | 23.8 |
| Tobacco | Note F: too unreliable to be published | Note ...: not applicable | Note ...: not applicable | Note F: too unreliable to be published | Note ...: not applicable | Note ...: not applicable | 21.5 | 15.5 | 29.0 |
| Other (flavourless, no usual flavour, alcohol, other) | 16.2Note E: Use with caution | 11.4 | 22.7 | 14.1Note E: Use with caution | 9.0 | 21.6 | 20.5Note E: Use with caution | 12.8 | 31.2 |
|
... not applicable E use with caution F too unreliable to be published
|
|||||||||
Substance use, peer behaviour and employment are risk factors for vaping in both age groups
Data from the 2019 CHSCY indicate that about three-quarters of adolescents aged 15 to 17 who reported consuming cannabis or tobacco products also reported vaping in the past 30 days (74.2% and 78.4%, respectively) (Table 1). In contrast, the prevalence of vaping was lower among non-smoking (tobacco) youth and those reporting never trying cannabis or infrequent cannabis use (17.1% and 16.0%, respectively). Similar patterns were observed for alcohol: about 4 in 10 (42.8%) of 15- to 17-year-olds reported vaping if they also reported drinking in the past year, compared with 5.1% if alcohol use was not reported.
Having many close friends who skipped school regularly, had reputations for causing trouble, drank or thought it was okay to not work hard in school (referred to as negative behaviours) was related to vaping in the past 30 days. For example, about a third (35.5%) of adolescents aged 15 to 17 reported vaping if many of their friends regularly engaged in one or more of the four behaviours, compared with 8.8% of those whose friends did not.
At 26.7%, the prevalence of vaping was about three times higher among youth aged 15 to 17 who had worked in the past year than it was among those who did not (10.8%).
Among younger adolescents aged 12 to 14, the consumption of tobacco, cannabis and alcohol; employment; and having many friends who engaged in least one of four negative behaviours was also associated with higher vaping prevalence compared with youth without these characteristics.
When other potentially influential variables such as sociodemographic characteristics, youth, parenting and peer factors were taken into account, the use of other substances (cannabis, tobacco and alcohol) for 15- to 17-year-olds or alcohol for 12- to 14-year-olds (sample size prevented inclusion of other substances in model) remained strongly associated with vaping (Table 4). Having friends who engaged in negative behaviours as well as employment remained risk factors for vaping among youth of both ages.
| Characteristics | 12 to 14 years | 15 to 17 years | ||||
|---|---|---|---|---|---|---|
| Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
|||
| from | to | from | to | |||
| Sociodemographic | ||||||
| Sex | ||||||
| Male | 0.8 | 0.6 | 1.2 | 1.6Note * | 1.3 | 2.0 |
| FemaleTable 4 Note ‡ | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Family structure (child lives with) | ||||||
| Two biological parents | 0.7 | 0.5 | 1.1 | 1.1 | 0.8 | 1.4 |
| OtherTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Canadian-born | ||||||
| Yes | 1.9 | 0.9 | 4.3 | 1.9Note * | 1.3 | 2.8 |
| No, including landed and non-permanent residentsTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Indigenous identity | ||||||
| Indigenous | 0.8 | 0.4 | 1.4 | 0.9 | 0.6 | 1.4 |
| Non-IndigenousTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Household income | ||||||
| Less than $40,000† | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| $40,000 to less than $100,000 | 0.9 | 0.5 | 1.6 | 1.0 | 0.7 | 1.4 |
| $100,000 or more | 1.4 | 0.8 | 2.4 | 1.0 | 0.7 | 1.4 |
| Youth, parenting and peer | ||||||
| Mood or anxiety disorder | ||||||
| Yes | 1.1 | 0.6 | 1.8 | 1.0 | 0.8 | 1.4 |
| NoTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Attention deficit hyperactivity disorder | ||||||
| Yes | 2.5Note * | 1.4 | 4.5 | 0.8 | 0.5 | 1.2 |
| NoTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Worked in the past 12 months | ||||||
| Yes | 1.5Note * | 1.0 | 2.2 | 1.4Note * | 1.1 | 1.8 |
| NoTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Overall mark in school | ||||||
| Mainly ATable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Lower than A | 1.5 | 1.0 | 2.1 | 1.4Note * | 1.1 | 1.7 |
| Children's Intrinsic Needs Satisfaction Scale | ||||||
| Relatedness subscale (continuous) | 0.4Note * | 0.2 | 0.7 | 0.9 | 0.6 | 1.3 |
| Competence subscale (continuous) | 1.0 | 0.6 | 1.8 | 0.9 | 0.6 | 1.2 |
| Autonomy subscale (continuous) | 1.4 | 0.9 | 2.2 | 0.9 | 0.7 | 1.2 |
| Alcohol use (past 12 months) | ||||||
| Regular or occassional use | 12.0Note * | 8.0 | 17.9 | 7.7Note * | 5.9 | 10.0 |
| Not in the past 12 months or never had a drinkTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Cigarettes or other tobacco use (past 30 days) | ||||||
| YesTable 4 Note † | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | 6.6Note * | 4.0 | 10.9 |
| No | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Cannabis use (past 30 days) | ||||||
| At least monthly | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | 3.4Note * | 2.3 | 5.0 |
| Once or twice, or neverTable 4 Note † | Note ...: not applicable | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Parents knew who child was with outside home | ||||||
| Frequently | 0.4Note * | 0.3 | 0.7 | 0.8 | 0.6 | 1.2 |
| Infrequently or not at allTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Spends time just talking with parents | ||||||
| Frequently | 1.1 | 0.6 | 1.9 | 1.1 | 0.8 | 1.5 |
| Infrequently or not at allTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Family member smokes (cigarettes, cigars or pipe tobacco) | ||||||
| Yes | 1.4 | 1.0 | 2.1 | 1.2 | 0.9 | 1.6 |
| NoTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
| Number of friends engaged in selected behaviours | ||||||
| Most or all | 1.9Note * | 1.3 | 2.7 | 2.2Note * | 1.8 | 2.8 |
| None or someTable 4 Note † | 1.0 | Note ...: not applicable | Note ...: not applicable | 1.0 | Note ...: not applicable | Note ...: not applicable |
... not applicable
|
||||||
Other characteristics associated with vaping differed by age
Among 15- to 17-year-olds, vaping was more common for males (23.4%) than females (19.0%) and those born in Canada (24.3%) versus the foreign-born (7.9%). School performance was also related to vaping, with use being about twice as common among students who did not receive mainly A-grades compared with those who did (27.3% versus 15.4%, respectively).
Vaping prevalence was higher among adolescents aged 12 to 14 who had been diagnosed with ADHD than those without ADHD (12.6% versus 4.7%). By contrast, having parents who usually knew who they were with when not home and higher relatedness scores (indicating a greater sense of belonging) were each protective and associated with lower levels of vaping.
Being male (Adjusted odds ratio (AOR) 1.6), Canadian-born (AOR 1.9) and having overall grades in school below A (AOR 1.4) were each significant vaping risk factors in the multivariable analysis of 15- to 17-year-olds. For 12- to 14-year-olds, having been diagnosed with ADHD (AOR 2.5) was a significant predictor of e-cigarette use, while better parental awareness of who the child is with (AOR 0.4) and higher relatedness scores (AOR 0.4) were associated with significantly lower odds of vaping.
Among both age groups, having a family member who smoked or having a mood or anxiety diagnosis appeared to increase the likelihood of vaping, but once other factors was taken into account, the associations were no longer significant.
Discussion
This study uses data from three nationally representative Canadian surveys to examine vaping prevalence and the unadjusted (bivariate) and adjusted associations of sociodemographic, youth, parenting and peer characteristics on vaping risk among younger and older adolescents.
Vaping has grown in popularity since the devices were first introduced to North AmericaNote 4 and is more common among adolescents than adults.Note 12Note 15 According to the 2019 CHSCY, 5.4% of 12- to 14-year-olds and 21.3% of 15- to 17-year-olds reported vaping in the past 30 days. Data from the 2019 CTNS suggest most e-cigarette users consume e-liquids containing nicotine, regardless of age.
Consistent with other research, data from the 2019 CTNS also found that candy-, dessert- and fruit-flavoured e-liquids were more popular among 15- to 19-year-olds than those aged 25 or older.Note 32 This is anticipated to change in response to the federal government’s proposal to ban the sale of most flavoursNote 33 and because some provinces (including, New BrunswickNote 34 and Prince Edward IslandNote 35) have already enacted bans in an effort to make vaping less attractive to youth.
Of additional concern are adolescents who used both e-cigarettes and tobacco cigarettes and, consequently, had greater exposure to nicotine and risk of dependence.Note 36 While the CHSCY did not ask about the age of first use of each tobacco product, the 2020 CCHS RR did and showed that about two-thirds of 12- to 17-year-olds and a third of 18- to 24-year-olds used e-cigarettes before trying their first regular cigarette. While some proportion of adolescents may have simply been experimenting with both products, other research has shown that e-cigarette users are at high risk of progressing to tobacco smoking.Note 16Note 19Note 20Note 23Note 37 A cohort effect related to the increasing availability of e-cigarettes over time may help explain why fewer 18- to 24-year-olds than 12- to 17-year-olds reported trying e-cigarettes first. That is, e-cigarettes may have been more accessible to the 12-to 17-year-olds in 2020 when they started to experiment than in earlier years when those currently comprising the older group would have been experimenting.
The association between other substance use (including tobacco, cannabis and alcohol) and vaping, has been found previously.Note 20Note 23Note 38Note 39 These associations remained significant even after controlling for sociodemographic, youth, parenting and peer characteristics among older adolescents. Similar results were found among 12- to 14-year-olds using alcohol. However, owing to the more limited sample and lower prevalence of cannabis and tobacco use for this age group, it was not possible to include these variables in the multivariable analysis.
There is also some uncertainty about the direction of the relationship between vaping and other substance use. It might be that vaping leads to other substance use, although the reverse is also possible. Additionally, it is thought that substance use behaviours cluster together,Note 40 or that some people are more prone to use drugs or engage in risky behaviours.Note 41Note 42
This study also found that adolescents in both age groups who had worked for money were more likely to vape than others who did not. It might be that the wages make vaping affordable for adolescents and that employed adolescents have more exposure to (often older) coworkers who vape. Other studies have found that more spending money increases vaping risk among adolescents.Note 38Note 43
Peer influence and social environment also affect adolescent substance use.Note 24Note 40Note 44Note 45Note 46Note 47Note 48 In this study, younger and older adolescents who reported having many friends who skipped school, used alcohol, had bad reputations, or thought it was okay to not work hard at school had about double the odds of vaping compared with other adolescents whose friends did not report these behaviours. For older adolescents, lower grades remained significantly associated with vaping in the multivariable analysis, consistent with others’ findings showing youth attending more academically focused programs were at reduced risk of vapingNote 47 as were adolescents reporting above-average academic performance.Note 49 By contrast, 12- to 14-year-olds with higher scores in relatedness (indicating a greater sense of closeness and belonging with others) had lower odds of vaping. This is similar to a finding from another study showing that higher relatedness was associated with lower odds of substance use for students from various grades.Note 50
A unique contribution of this study is that data were included for both younger and older adolescents, enabling comparison by age. While some of the factors associated with vaping (in the adjusted models) were important for both age groups (alcohol use, employment and having friends who engaged in negative behaviours), others were pertinent to just one (sex, country of birth, grades, tobacco and cannabis use, ADHD, parents knowing who you are with, and relatedness). Knowing more about which risk factors matter according to age group could be used to tailor anti-vaping and related educational materials. Additionally, some of the risk factors identified are potentially modifiable or appropriate for awareness campaigns.
Consistent with previous work,Note 23Note 24Note 46Note 47Note 51 this study found that 15-to 17-year-old boys were more likely to have vaped than similarly aged girls. In this study, Canadian-born adolescents aged 15 to 17 also had greater odds of vaping than youth born elsewhere, similar to American findings that immigrants were less likely to vape than those born in the United States.Note 52
This study found that vaping risk for younger adolescents was significantly reduced when they reported that their parents usually knew who they were with when not home. This supports previous research suggesting that parental supervision is an important factor in the prevention of substance use.Note 44Note 49
Another finding was that a diagnosis of ADHD among 12- to 14-year-olds was associated with increased odds of vaping. This accords with other research and may be related to difficulties with attention, impulsivity and decision making; characteristic of the condition; or possibly the use of vaping (nicotine) as a form of self-medication and symptom management.Note 53Note 54Note 55Note 56
Strengths and limitations
This study has a number of strengths, including the use of three nationally representative and recent Canadian data sources which allow for a more fulsome evaluation of vaping among Canadian adolescents as young as age 12. The CHSCY included a comprehensive range of covariates permitting an examination of the simultaneous contribution of youth, peer group and parental characteristics not normally possible with other data sources. Nevertheless, results of this study should be interpreted in light of several limitations.
The data are cross-sectional and so permit the observation of associations between variables at only one point in time and do not allow for causal inference. Information from the surveys was self-reported and has not been verified and can be subject to recall and social desirability biases.
While both the CTNS and CCHS RR on smoking stages of change, tobacco alternatives and vaping specifically instructed respondents to exclude the vaping of cannabis when answering the vaping questions. A similar qualifying statement was not included in the CHSCY. It is not known whether respondents of any of the surveys used in this study included the vaping of cannabis in their responses, as the data were self-reported. This could result in an overestimate of the prevalence of vaping, although the impact is expected to be minimal because cannabis use is comparatively low in those under the age of 18.Note 57
Some variables relevant to the study of adolescent vaping were not collected in CHSCY, including the perception of risk or harm from vaping, exposure to advertising, whether friends or family vape, or the specifics of the devices used and ingredients of the e-liquids. The provincial samples were not large enough to consider differences in use or emerging regulatory differences by province.
Data were collected before the implementation of new and proposed regulatory policies limiting the amount of nicotine and flavours in e-cigarettes.Note 33Note 34Note 35 Thus, research could be undertaken to evaluate the impact of these changes on adolescent vaping in the future.
While the CHSCY was designed to study the health of children and youth and boasts a comparatively large sample, the problem of small sample sizes was not completely eliminated and sometimes necessitated the collapsing of covariate categories or even the removal of some variables from regressions. Analysis by different racialized groups was attempted, but the available sample necessitated the variable be dichotomized (White only versus non-White) rather than retaining various racial identities (e.g., Black or Chinese). Given the similarity of results to those of the immigrant versus Canadian-born variable and considerable overlap between the two, the decision was made to select the immigrant–Canadian-born results for study inclusion. Small samples or effect sizes in other parts of the analysis may also have impacted significance testing.
Conclusion
The study provides a comprehensive picture of factors associated with vaping among both younger and older adolescents in Canada.
Findings highlight the importance of relationships and friend behaviours on adolescent vaping. Also important are sex, country of birth, employment, ADHD and school grades. For some characteristics, the susceptibility to the risk of vaping differed by age. The strong associations with alcohol, tobacco and cannabis use suggest that efforts to reduce vaping might also include measures to reduce use of other substances.
The findings about correlates of adolescent vaping could inform prevention and regulatory policy in an effort to reduce the attractiveness of e-cigarettes in the hopes of preventing the future burden of vaping-related disease on young Canadians.
Factors such as changing regulatory environments and the COVID-19 pandemic could impact the prevalence of adolescent vaping beyond the 2019/2020 time frame of this study. Thus, additional monitoring is necessary to identify ongoing changes.
- Date modified: