
 StatCan COVID-19: The effect of COVID-19 on physical activity among Canadians and the future risk of cardiovascular disease
StatCan COVID-19: The effect of COVID-19 on physical activity among Canadians and the future risk of cardiovascular disease

Archived Content
Information identified as archived is provided for reference, research or recordkeeping purposes. It is not subject to the Government of Canada Web Standards and has not been altered or updated since it was archived. Please "contact us" to request a format other than those available.
by Douglas G. Manuel, Anan Bader Eddeen, Rachel C. Colley, Michael Tjepkema, Rochelle Garner, Carol Bennett and Julie Bernier
Skip to text
Acknowledgements
We would like to thank Tracey Bushnik, Evelyne Bougie and Thomas Charters for conducting a literature review on changes in health risk behaviours since the start of the pandemic. We would also like to thank Heather Gilmour for analytical support.
Introduction
Prevention and control measures implemented since March 2020 in response to the COVID-19 pandemic have changed how Canadians live. In an effort to slow the spread of COVID-19, Canadians have limited their contact with people outside their household, businesses have shifted from in-person to online interactions, the prevalence of working from home has increased, students have been attending school remotely and social interactions have become physically distanced (Leclerc 2020; Gilmour 2020; Savage and Turcotte 2020; Deng, Morissette and Messacar 2020).
The shift by Canadians to a more physically distanced life resulted in a dramatic reduction in the transmission of COVID-19. However, there are concerns that health behaviours, including physical activity, have consequently changed in ways that will result in an unintended increase in the risk of chronic diseases such as cardiovascular disease, obesity, diabetes and cancer.
The benefits of physical activity are well known and include lowering the risk of death and the risk of developing cardiovascular disease (e.g., heart disease and stroke), diabetes, depression, anxiety, dementia, several types of cancers and other conditions (Ross et al. 2020). There is strong evidence of an inverse dose–response relationship between physical activity and the risk of cardiovascular disease, with the greatest preventive benefit observed for individuals moving from no or little physical activity to some physical activity (Physical Activity Guidelines Advisory Committee 2008; Ross et al. 2020; Sattelmair et al. 2011). There is approximately a 14% reduction in cardiovascular disease for people who meet the Canadian recommendations for physical activity, i.e., 150 minutes of moderate to vigorous physical activity per week (Ross et al. 2020), compared with people who are inactive (Arem et al. 2015; Sattelmair et al. 2011).
This study looks at how many Canadians could potentially develop cardiovascular disease over the next three years because of reduced levels of physical activity during the COVID-19 pandemic. Based on small Canadian studies and international research indicating that physical activity has declined during the pandemic, the authors use three hypothetical scenarios to reflect a possible range of changes in physical activity levels—reductions of 10%, 20% and 40%—in addition to a fourth scenario, no change in activity. Whether these reductions apply equally to all population groups is not known. Further, some groups may have increased physical activity levels. These scenarios describe the potential impact on cardiovascular disease by different levels of physical activity reductions. A three-year period was used in order to illustrate the possible longer-term impact of decreased physical activity. If Canadians return to their normal level of physical activity in fewer years, there would be a corresponding reduction in the number of people that could develop cardiovascular disease over three years.
Physical activity prior to and during the COVID-19 pandemic
Although lockdown periods and physical distancing measures have been critical to reducing virus transmission, prolonged restrictions may have decreased opportunities for exercise for Canadians as a whole, or for specific population groups.. People have been spending more time at home, which has resulted in them spending less time doing common types of physical activity such as walking or biking to work, organized sports and recreational activities: in some cases, these activities were cancelled altogether. At the same time, it is possible that some people may have replaced some of these activities with others that allowed for social distancing, such as cycling and running. Prior to the onset of the COVID-19 pandemic, less than half of Canadian adults met the physical activity recommendation of 150 minutes of moderate to vigorous physical activity per week (Bethell et al. 2019). Evidence from international research (Ammar et al. 2020; Caputo and Reichert 2020; Fitbit 2020; Flanagan et al. 2021; Meyer et al. 2020; Violant-Holz et al. 2020) and Canadian research (Di Sebastiano et al. 2020; Lesser and Nienhuis 2020; Woodruff, Coyne and St-Pierre 2021) suggests that, in general, adults have decreased their level of physical activity and increased the amount of time spent sitting during the COVID-19 pandemic.
The risk of cardiovascular disease before and during the pandemic
Table 1 shows that the three-year multivariable risk of cardiovascular disease for Canadians increases with age. Prior to the COVID-19 pandemic, many Canadian adults were at risk of developing cardiovascular disease because of low levels of physical activity. At pre-pandemic levels of physical activity, approximately 228,200 Canadians were expected to develop cardiovascular disease during the three-year period from March 2020 to March 2023.
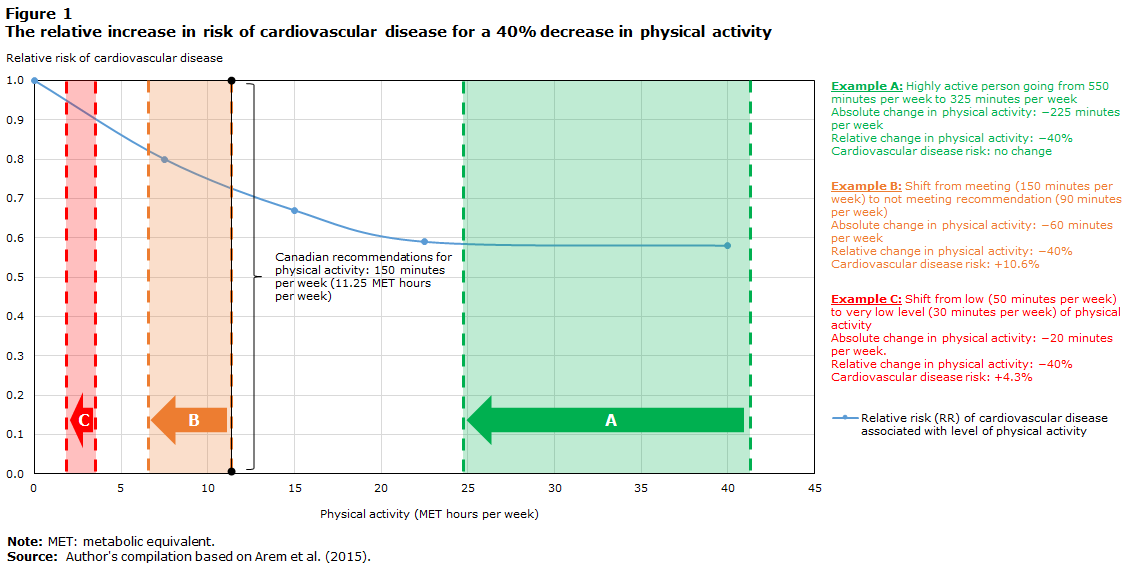
Figure 1 presents three examples of how a person’s risk of developing cardiovascular disease increases when their level of physical activity decreases by 40%, according to a meta-analysis by Arem et al. (2015). Example A represents a highly active person at baseline. If this person previously exceeded the recommended level of physical activity, for example, 550 minutes, or 41.3 metabolic equivalent (MET) hours, per week, the risk of cardiovascular disease does not change when their physical activity decreases by 40% (i.e., to 325 minutes, or 24.8 MET hours, per week). In example B (a person who just meets the physical activity recommendation at baseline), the risk of cardiovascular disease increases by 10.6% when their physical activity decreases by 40% (i.e., from 150 minutes, or 11.3 MET hours, per week to 90 minutes, or 6.8 MET hours, per week). In example C (a person below the recommendation at baseline), the risk of cardiovascular disease increases by 4.3% when their physical activity decreases by 40% (i.e., from 50 minutes, or 3.8 MET hours, per week to 30 minutes, or 2.3 MET hours, per week).
| Age Group | Number of Canadians | 3-year CVD risk | New cases of CVD, 2020 to 2023 |
|---|---|---|---|
| number | percent | number | |
| Women, aged 20 and older | 13,339,000 | 0.68 | 90,500 |
| 20 to 39 | 4,651,000 | 0.03 | 1,600 |
| 40 to 59 | 4,738,000 | 0.30 | 14,100 |
| 60 to 79 | 3,405,000 | 1.40 | 47,700 |
| 80 or older | 545,000 | 5.00 | 27,000 |
| Men, aged 20 and older | 12,879,000 | 1.10 | 137,700 |
| 20 to 39 | 4,863,000 | 0.10 | 3,000 |
| 40 to 59 | 4,699,000 | 0.90 | 41,300 |
| 60 to 79 | 2,921,000 | 2.40 | 71,400 |
| 80 or older | 395,000 | 5.60 | 22,000 |
|
Note: CVD: Cardiovascular disease. Numbers may not sum to the total because of rounding. Sources: Statistics Canada, 2018 Canadian Community Health Survey, Cardiovascular Population Risk Tool (CVDPoRT). |
|||
Description of figure 1
La figure 1 présente le lien entre l’activité physique et le risque de maladie cardiovasculaire utilisé dans la présente étude. La ligne courbe a été créée à partir des données figurant au tableau 3 d’une analyse groupée effectuée par Hannah Arem et ses collègues et publiée en 2015. La dose d’activité physique est présentée comme étant le nombre d’heures MET par semaine (axe des X) et le risque de maladie cardiovasculaire est présenté comme étant un risque relatif (axe des Y). L’acronyme MET signifie équivalent métabolique et représente la dépense énergétique. À titre de référence, 1 MET représente la dépense énergétique d’une personne au repos. La forme de la courbe illustre une forte pente descendante suivie d’un long plateau. Cela signifie qu’une légère augmentation de l’activité physique chez les personnes inactives ou peu actives entraîne une diminution plus importante du risque de maladie cardiovasculaire (c.-à-d. dans la partie abrupte de la courbe) comparativement à l’incidence sur le risque lorsqu’une personne très active augmente son niveau d’activité physique (c.-à-d. dans le plateau de la courbe).
La figure 1 présente trois exemples de la façon dont le risque de maladie cardiovasculaire d’une personne augmente lorsque son niveau d’activité physique diminue de 40 %, selon une méta-analyse effectuée par Arem et coll. (2015).
L’exemple A représente une personne très active au départ. Si cette personne a déjà dépassé le niveau d’activité physique recommandé, par exemple, 550 minutes ou 41,3 heures d’équivalent métabolique (MET) par semaine, le risque de maladie cardiovasculaire ne change pas lorsque son niveau d’activité physique diminue de 40 % (c.-à-d. une diminution de 225 minutes à 325 minutes, ou 24,8 heures MET, par semaine).
Dans l’exemple B (une personne qui ne fait que respecter la recommandation en matière d’activité physique au départ), le risque de maladie cardiovasculaire augmente de 10,6 % lorsque son niveau d’activité physique diminue de 40 % (c.-à-d. lorsqu’elle passe de 150 minutes, ou 11,3 heures MET, par semaine, à 90 minutes, ou 6,8 heures MET, par semaine, soit une diminution 60 minutes).
Dans l’exemple C (une personne dont le niveau d’activité physique est inférieur à la recommandation au départ), le risque de maladie cardiovasculaire augmente de 4,3 % lorsque son activité physique diminue de 40 % (c.-à-d. lorsqu’elle passe de 50 minutes, ou 3,8 heures MET, par semaine, à 30 minutes, ou 2,3 heures MET, par semaine, soit une diminution de 20 minutes).
Table 2 shows how many more people are predicted to be diagnosed with cardiovascular disease between 2020 and 2023 under three scenarios of change in physical activity: reductions of 10%, 20% and 40%. These scenarios represent a range of plausible changes in leisure-time activity levels during the pandemic. Depending on the scenario, the number of people diagnosed with cardiovascular disease over a three-year period would increase by 1,600 to 4,800.
| Age Group | Number of Canadians | No change in physical activity | |||
|---|---|---|---|---|---|
| 10% decrease | 20% decrease | 40% decrease | |||
| number | |||||
| Women, aged 20 and older | 13,339,000 | 90,500 | 534 | 600 | 1,481 |
| 20 to 39 | 4,651,000 | 1,600 | 14 | 19 | 46 |
| 40 to 59 | 4,738,000 | 14,100 | 123 | 137 | 360 |
| 60 to 79 | 3,405,000 | 47,700 | 320 | 354 | 872 |
| 80 or older | 545,000 | 27,000 | 81 | 87 | 209 |
| Men, aged 20 and older | 12,879,000 | 137,700 | 1,133 | 1,288 | 3,361 |
| 20 to 39 | 4,863,000 | 3,000 | 34 | 34 | 102 |
| 40 to 59 | 4,699,000 | 41,300 | 400 | 451 | 1,175 |
| 60 to 79 | 2,921,000 | 71,400 | 602 | 689 | 1,823 |
| 80 or older | 395,000 | 22,000 | 100 | 110 | 269 |
|
Note: Numbers may not sum to the total because of rounding. Sources: Statistics Canada, 2018 Canadian Community Health Survey, Cardiovascular Population Risk Tool (CVDPoRT). |
|||||
Methodology
The analyses were conducted in three steps.
First, data from the 2018 Canadian Community Health Survey (CCHS) were used to estimate the prevalence of leisure-time physical activity and other cardiovascular risk factors prior to the COVID-19 pandemic. The CCHS was the most complete data source available for estimating pre-pandemic levels of behaviours and health.
Second, the probability of being diagnosed with cardiovascular disease in the next three years was calculated for each CCHS respondent using the Cardiovascular Population Risk Tool (CVDPoRT). The CVDPoRT is a predictive risk algorithm developed and validated by linking earlier cycles of the CCHS (i.e., 2001 to 2012) to cardiovascular hospitalization and death records (Manuel et al. 2018). To calculate cardiovascular risk, a total of 12 risk factors were used: age, sex, ethnicity, immigrant status and education (sociodemographic characteristics); smoking, alcohol consumption, diet and physical activity (health behaviours); diabetes and high blood pressure (previously diagnosed chronic conditions); and body mass index. The total number of new cardiovascular events was the weighted sum of the CVDPoRT risk calculated at baseline (i.e., the 2018 CCHS) for respondents aged 20 or older.
Third, the relative change in cardiovascular risk associated with a change in physical activity was estimated from a meta-analysis of published studies (Arem et al. 2015). Figure 1 presents the relationship between physical activity and cardiovascular disease risk used in this current study.
To estimate the potential increase in new cardiovascular events, the three estimates—physical activity, cardiovascular disease risk and the relative change in cardiovascular disease risk—were multiplied for each 2018 CCHS respondent aged 20 or older. Four different scenarios (no change, −10%, −20% and −40%) were examined (Table 2). The leisure-time physical activity level of each CCHS respondent was altered according to the scenario and the cardiovascular disease risk recalculated (Manuel 2013; Manuel et al. 2016), with all other characteristics remaining unchanged. The number of new cases of cardiovascular disease that could be attributed to reduced physical activity levels in a given scenario was the weighted sum of the new cardiovascular disease events subtracted from the baseline risk scenario (i.e., unchanged physical activity levels as reported in the 2018 CCHS). For example, if a respondent reported they walked 60 minutes a day, their leisure-time physical activity would be 2 MET hours per day. In the scenario of 20% reduction in leisure-time physical activity, the value would be reduced to 1.6 MET hours per day. The increase in the respondent’s risk of cardiovascular disease from reduced physical activity was calculated by multiplying the relative risk increase of 0.4 MET hours, as seen in Figure 1, by the respondent’s baseline cardiovascular disease risk.
Discussion
Stay-at-home and other restrictions may increase the long-term risk of cardiovascular disease associated with an unhealthy lifestyle (Mattioli et al. 2020). Promoting the importance of maintaining a regular exercise routine during periods of lockdown may help prevent cardiovascular disease and other long-term chronic diseases associated with unhealthy lifestyle habits. Promoting adequate levels of physical activity is important for reducing the estimated number of new cases of cardiovascular disease over the three-year period reported in this study.
These preliminary results are based on hypothetical decreases in physical activity during the COVID-19 pandemic. Although the precise impact of the COVID-19 pandemic on Canadians’ physical activity is unknown and whether this impact varies by population group, a growing body of evidence suggests that an overall reduction in activity levels has occurred. Throughout the pandemic, the CCHS has been collecting data on Canadians’ level of physical activity, diet, smoking and alcohol consumption habits, and mental health. The lifestyle and health trends can be further examined using Statistics Canada’s Population Health Model (POHEM), which goes beyond the analyses presented in this report to include multiple risks and chronic diseases (Hennessy et al. 2015). Future POHEM analyses can address the limitations of this study and several assumptions, for example, that cardiovascular risk is the same in 2020, at the beginning of the pandemic, as in 2018. Using a model like POHEM would also allow researchers to examine changes in multiple risk factors together, for example, body weight and physical activity. Collection of data one year post-COVID will be essential to identify the changes who persist over time.
This present study highlights the important role physical activity has on the incidence of cardiovascular disease among Canadian adults. Decreases in levels of physical activity could lead to an increased incidence of cardiovascular disease in the population, particularly among those who are already inactive or who go from meeting to not meeting the current Canadian recommendations for physical activity.
References
Ammar, A., M. Brach, K. Trabelsi, H. Chtourou, O. Boukhris, L. Masmoudi, B. Bouaziz, E. Bentlage, D. How, and M. Ahmed. 2020. “Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey.” Nutrients 12 (6): 1583.
Arem, H., S.C. Moore, A. Patel, P. Hartge, A. Berrington de Gonzalez, K. Visvanathan, P.T. Campbell, M. Freedman, E. Weiderpass, H.O. Adami, M.S. Linet, I-M. Lee, and C.E. Matthews. 2015. “Leisure time physical activity and mortality: A detailed pooled analysis of the dose–response relationship.” JAMA Internal Medicine 175 (6): 959–967. Available at: https://doi.org/10.1001/jamainternmed.2015.0533.
Bethell, J., M.T.E. Puts, S. Sattar, M.K. Andrew, A.S. Choate, B. Clarke, K. Cowan, C. DeAngelis, J. Elliott, M.I. Fitch, C. Frank, K. Hominick, M. Keatings, J.E. McElhaney, S.M. McKay, E. Pitters, J. Ploeg, S. Sidani, and K.S. McGilton. 2019. “The Canadian Frailty Priority Setting Partnership: Research priorities for older adults living with frailty.” Canadian Geriatrics Journal 22 (1): 23–33. Available at: https://doi.org/10.5770/cgj.22.336.
Caputo, E.L., and F.F. Reichert. 2020. “Studies of physical activity and COVID-19 during the pandemic: A scoping review.” Journal of Physical Activity and Health 17 (12): 1275–1284.
Deng, Z., R. Morissette, and D. Messacar. 2020. Running the Economy Remotely: Potential for Working from Home During and After COVID-19. StatCan COVID-19: Data to Insights for a Better Canada. Statistics Canada Catalogue no. 45-28-0001. Ottawa: Statistics Canada.
Di Sebastiano, K.M., T. Chulak-Bozzer, L.M. Vanderloo, and G. Faulkner. 2020. “Don’t walk so close to me: Physical distancing and adult physical activity in Canada.” Frontiers in Psychology 11: 1895.
Fitbit. “The impact of coronavirus on global activity.” Fitbit News, March 23, 2020. Available at: https://blog.fitbit.com/covid-19-global-activity/.
Flanagan, E.W., R.A. Beyl, S.N. Fearnbach, A.D. Altazan, C.K. Martin, and L.M. Redman. 2021. “The impact of COVID-19 stay-at-home orders on health behaviors in adults.” Obesity 29 (2): 438–445.
Gilmour, H. 2020. Self-Perceived Mental Health and Health-Related Behaviours of Canadians During the COVID-19 Pandemic. StatCan COVID-19: Data to Insights for a Better Canada. Statistics Canada Catalogue no. 45-28-0001. Ottawa: Statistics Canada.
Hennessy, D.A., W.M. Flanagan, P. Tanuseputro, C. Bennett, M. Tuna, J. Kopec, M.C. Wolfson, and D.G. Manuel. 2015. “The Population Health Model (POHEM): An overview of rationale, methods and applications.” Population Health Metrics 13: 24. Available at: https://doi.org/10.1186/s12963-015-0057-x.
Leclerc, K. 2020. Caring for Their Children: Impacts of COVID-19 on Parents. StatCan COVID-19: Data to Insights for a Better Canada. Statistics Canada Catalogue no. 45-28-0001. Ottawa: Statistics Canada. Available at: https://www150.statcan.gc.ca/n1/en/pub/45-28-0001/2020001/article/00091-eng.pdf?st=lUKjhtKj.
Lesser, I.A., and C.P. Nienhuis. 2020. “The impact of COVID-19 on physical activity behavior and well-being of Canadians.” International Journal of Environmental Research and Public Health 17 (11): 3899.
Manuel, D.G. 2013. “The burden of unhealthy living in Ontario: The impact of smoking, alcohol, diet, physical inactivity and stress on life expectancy.” Healthcare Quarterly 16 (1): 16–18.
Manuel, D.G., R. Perez, C. Sanmartin, M. Taljaard, D. Hennessy, K. Wilson, P. Tanuseputro, H. Manson, C. Bennett, M. Tuna, S. Fisher, and L.C. Rosella. 2016. “Measuring burden of unhealthy behaviours using a multivariable predictive approach: Life expectancy lost in Canada attributable to smoking, alcohol, physical inactivity, and diet.” PLOS Medicine 13 (8): e1002082. Available at: https://doi.org/10.1371/journal.pmed.1002082.
Manuel, D.G., M. Tuna, C. Bennett, D. Hennessy, L. Rosella, C. Sanmartin, J.V. Tu, R. Perez, S. Fisher, and M. Taljaard. 2018. “Development and validation of a cardiovascular disease risk-prediction model using population health surveys: The Cardiovascular Disease Population Risk Tool (CVDPoRT).” CMAJ 190 (29): E871–E882. Available at: https://doi.org/10.1503/cmaj.170914.
Mattioli, A.V., M.B. Puviani, M. Nasi, and A. Farinetti. 2020. “COVID-19 pandemic: The effects of quarantine on cardiovascular risk.” European Journal of Clinical Nutrition 74 (6): 852–855.
Meyer, J., C. McDowell, J. Lansing, C. Brower, L. Smith, M. Tully, and M. Herring. 2020. “Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults.” International Journal of Environmental Research and Public Health 17 (18): 6469. Available at: https://doi.org/10.3390/ijerph17186469.
Physical Activity Guidelines Advisory Committee. 2008. Physical Activity Guidelines Advisory Committee Report, 2008. Washington: U.S. Department of Health and Human Services.
Ross, R., J.-P. Chaput, L.M. Giangregorio, I. Janssen, T.J. Saunders, M.E. Kho, V.J. Poitras, J.R. Tomasone, R. El-Kotob, and E.C. McLaughlin. 2020. “Canadian 24-Hour Movement Guidelines for adults aged 18–64 years and adults aged 65 years or older: An integration of physical activity, sedentary behaviour, and sleep.” Applied Physiology, Nutrition, and Metabolism 45 (10): S57–S102.
Sattelmair, J., J. Pertman, E.L. Ding, H.W. Kohl, W. Haskell, and I-M. Lee. 2011. “Dose–response between physical activity and risk of coronary heart disease: A meta-analysis.” Circulation 124 (7): 789–795. Available at: https://doi.org/10.1161/CIRCULATIONAHA.110.010710.
Savage, K., and M. Turcotte. 2020. Commuting to Work During COVID-19. StatCan COVID-19: Data to Insights for a Better Canada. Statistics Canada Catalogue no. 45-28-0001. Ottawa: Statistics Canada. Available at: https://www150.statcan.gc.ca/n1/en/pub/45-28-0001/2020001/article/00069-eng.pdf?st=iVPL9AAS.
Violant-Holz, V., M.G. Gallego-Jiménez, C.S. González-González, S. Muñoz-Violant, M.J. Rodríguez, O. Sansano-Nadal, and M. Guerra-Balic. 2020. “Psychological health and physical activity levels during the COVID-19 pandemic: A systematic review.” International Journal of Environmental Research and Public Health 17 (24): 9419. Available at: https://doi.org/10.3390/ijerph17249419.
Woodruff, S.J., P. Coyne, and E. St-Pierre. 2021. “Stress, physical activity, and screen-related sedentary behaviour within the first month of the COVID-19 pandemic.” Applied Psychology: Health and Well-Being. Forthcoming. Available at: https://doi.org/10.1111/aphw.12261.
- Date modified: