
Portrait of Youth in Canada: Data Report
Chapter 1: Health of youth in Canada

Archived Content
Information identified as archived is provided for reference, research or recordkeeping purposes. It is not subject to the Government of Canada Web Standards and has not been altered or updated since it was archived. Please "contact us" to request a format other than those available.
Skip to text
Text begins
Start of text box
- Canadian youth aged 15 to 30 were in the best physical shape of their life: they were less likely to be obese, were more active and smoked less than older Canadians.
- Compared with 20 years earlier, a higher proportion of Canadian youth were obese, they were less active, and ate fewer servings of fruit and vegetables.
- Canadian youth reported worse mental health than older Canadians both before and during the COVID-19 pandemic. Their mental health was also poorer than it was 20 years ago.
- Heavy drinking and tobacco smoking have significantly decreased among youth over the last 20 years in Canada.
End of text box
Introduction
Eighty-five years old—this is the age a 25-year-old woman in 2020 is expected to reach. Her male counterpart is expected to live to 81 years of age. Life expectancy is an important summary measure of a nation’s health, and, in Canada, it has been increasing. Women aged 25 are expected to live 3.6 years longer than their mothers and 8.7 years longer than their grandmothers. For 25-year-old men, life expectancy is 5.8 years longer than for their fathers and 9.2 years longer than for their grandfathers.
Although life expectancy has been rising for everyone, some groups have made greater gains than others. For example, more affluent and more educated people have gained more years than those who are poorer and less educated, as has been shown in data from 1996 and 2011.Note 1 Indigenous people have gained years of life, but these have not kept up with those of the non-Indigenous population.Note 2
Using Statistics Canada data, this chapter goes beyond the measure of life expectancy to describe the health of Canadian youth, defined as those aged 15 to 30 years old. Indicators of physical and mental health and substance use are presented to highlight the health of young Canadians. Comparisons with older Canadians and trends mostly over the last 20 years are provided. When possible, indicators are also examined by sex, ethnicity and household income. The health of Indigenous youth is also important. However, to put results for this population in the proper context, a full chapter will be dedicated to Indigenous youth.
In March 2020, physical distancing began to be recommended and schools and businesses were closed to slow the spread of COVID-19. It is not possible to discuss health without examining the impact of these measures; this chapter also highlights some of the short-term consequences of COVID-19 on youth.
Physical health and behaviours
Age and sex
Self-perceived health, which is how people rate their own health, is an accurate indicator of overall health. In addition, behaviours and conditions such as cigarette smoking, obesity, physical activity, and fruit and vegetable consumption are strong predictors of an individual’s future health.
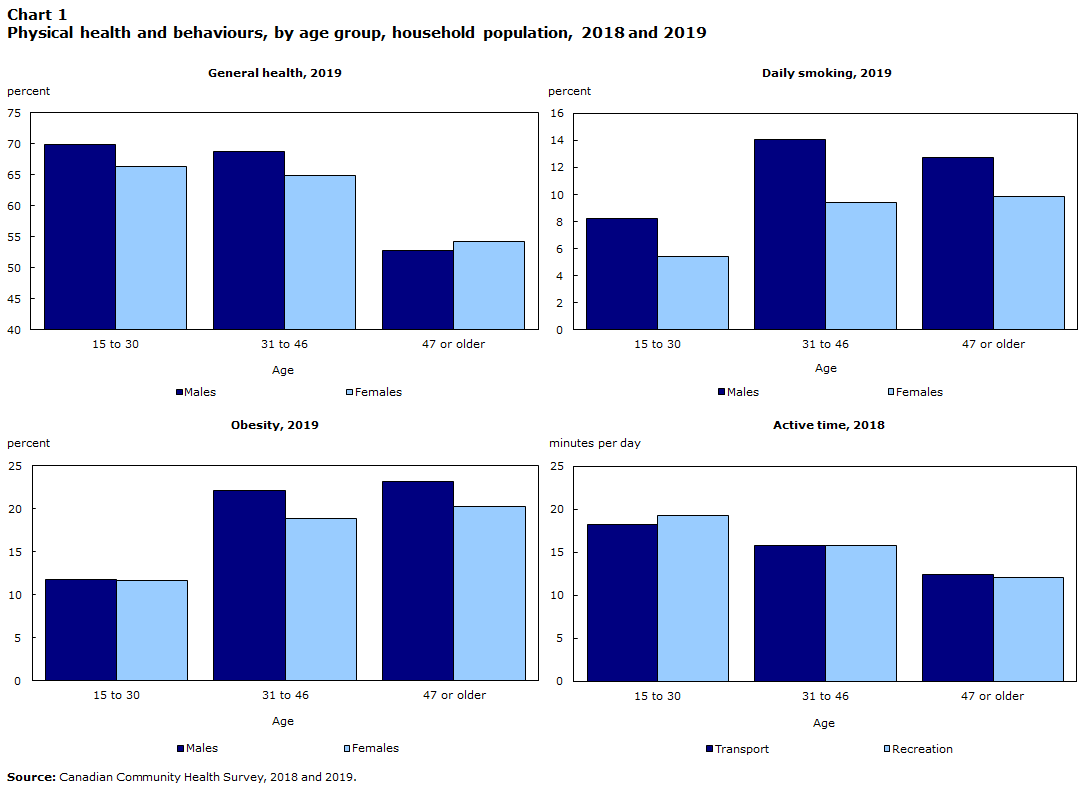
Compared with older Canadians, youth were in the best physical shape of their lives. They reported better health, smoked less (at least on a daily basis), were more active and were less likely to be obese than older Canadians (Chart 1). This was true for both males and females. However, there were some differences between young males and females: males reported slightly better general health, but were more likely to smoke on a daily basis. In addition, young males reported 6.6 more minutes per day, on average, of recreational physical activity than young females. No difference was observed for physical activity from transportation, and obesity rates did not differ for that younger age group.
Data table for Chart 1
| Age | General health, 2019 | Daily Smoking, 2019 | Obesity, 2019 | Active time, 2018 | ||||
|---|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | Transport | Recreation | |
| percent | minutes per day | |||||||
| 15 to 30 | 70.0 | 66.4 | 8.2 | 5.5 | 11.8 | 11.7 | 18.3 | 19.3 |
| 31 to 46 | 68.8 | 64.9 | 14.1 | 9.4 | 22.2 | 18.9 | 15.8 | 15.7 |
| 47 or older | 52.8 | 54.2 | 12.7 | 9.8 | 23.2 | 20.3 | 12.4 | 12.1 |
| Source: Canadian Community Health Survey, 2018 and 2019. | ||||||||
As of January 2021, more than 700,000 Canadians had tested positive for COVID-19.Note 3 Youth aged 20 to 29 years old accounted for 18.7% of these cases, a higher percentage than their demographic weight, i.e., their overall representation in the Canadian population. However, they were less likely to have been hospitalized or to have died from COVID-19. In early April 2020, a higher percentage of Canadians actually reported excellent or very good health than in 2018.Note 4 A majority of people aged 20 to 34 reported an increase in the amount of exercise they were doing, but also an increase in screen time.Note 5
Start of text box
As of January 8, 2021,*
- out of 631,980 COVID-19 cases with age information, 18.7% were in people aged 20 to 29, a proportion that has been increasing in fall 2020
- out of 35,154 hospitalizations, 3.1% were of people aged 20 to 29
- out of 6,448 intensive care unit admissions, 2.8% were of people aged 20 to 29
- out of 16,435 deaths, 0.1% were of people aged 20 to 29.
According to the 2016 Census, 20- to 29-year-olds represented 12.9% of the Canadian population.
*From the Public Health Agency of Canada daily epidemiological report.Note 3
End of text box
Longer-term trend
Although young Canadians reported better health than their older counterparts, not all indicators were positive. For example, obesity rates have been slowly increasing over the last 20 years for both males and females (Chart 2). More recently, physical activity and fruit and vegetable consumption have been decreasing (Chart 2). Young females consumed fruit and vegetables more often than males, but the trend was the same. The downward trend in recreational physical activity was driven by changes in the behaviour of young males.
By contrast, youth cigarette smoking rates have never been lower and have been steadily declining since 2001. Daily smoking rates went from nearly one-quarter (23.9%) in 2001 to 6.9% in 2019. When occasional smokers are added, rates went from 31.4% in 2001 to 14.8% in 2019. The trends were the same for both males and females (Chart 2).
However, vaping (or the use of e-cigarettes) has been gaining in popularity, and the latest data suggest it is considerably more popular among youth than the older population. An estimated 15% of youth aged 15 to 24 reported having vaped in the past 30 days when asked in 2019. By contrast, 3% of the population aged 25 and older reported having vaped.Note 6 This is a newer phenomenon that could affect smoking rates in the future.

Data table for Chart 2
| Year | Daily Smoking | Obesity | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| percent | ||||
| 2001 | 25.7 | 22.0 | 9.6 | 7.0 |
| 2003 | 22.1 | 18.6 | 10.5 | 8.1 |
| 2005 | 19.5 | 15.2 | 10.1 | 7.6 |
| 2007 to 2008 | 21.0 | 16.2 | 10.7 | 8.0 |
| 2009 to 2010 | 18.3 | 13.4 | 11.7 | 8.1 |
| 2011 to 2012 | 16.9 | 13.2 | 10.6 | 9.0 |
| 2013 to 2014 | 15.2 | 10.8 | 12.4 | 8.7 |
| 2015 to 2016 | 12.2 | 8.7 | 11.4 | 9.3 |
| 2017 to 2018 | 10.7 | 7.7 | 11.4 | 10.4 |
| 2019 | 8.2 | 5.5 | 11.8 | 11.7 |
| Fruit and vegetables | |||
|---|---|---|---|
| 2015 | 2016 | 2017 | |
| times consumed per day | |||
| Fruit and vegetables | 3.7 | 3.7 | 3.5 |
| Fruit juice | 0.5 | 0.4 | 0.4 |
| Active timeData table Note 1 | ||
|---|---|---|
| Transport | Recreation | |
| Year | minutes per day | |
| 2015 | 19.8 | 22.4 |
| 2016 | 21.6 | 22.5 |
| 2017 | 18.9 | 23.2 |
| 2018 | 18.3 | 19.3 |
|
||
Social determinants
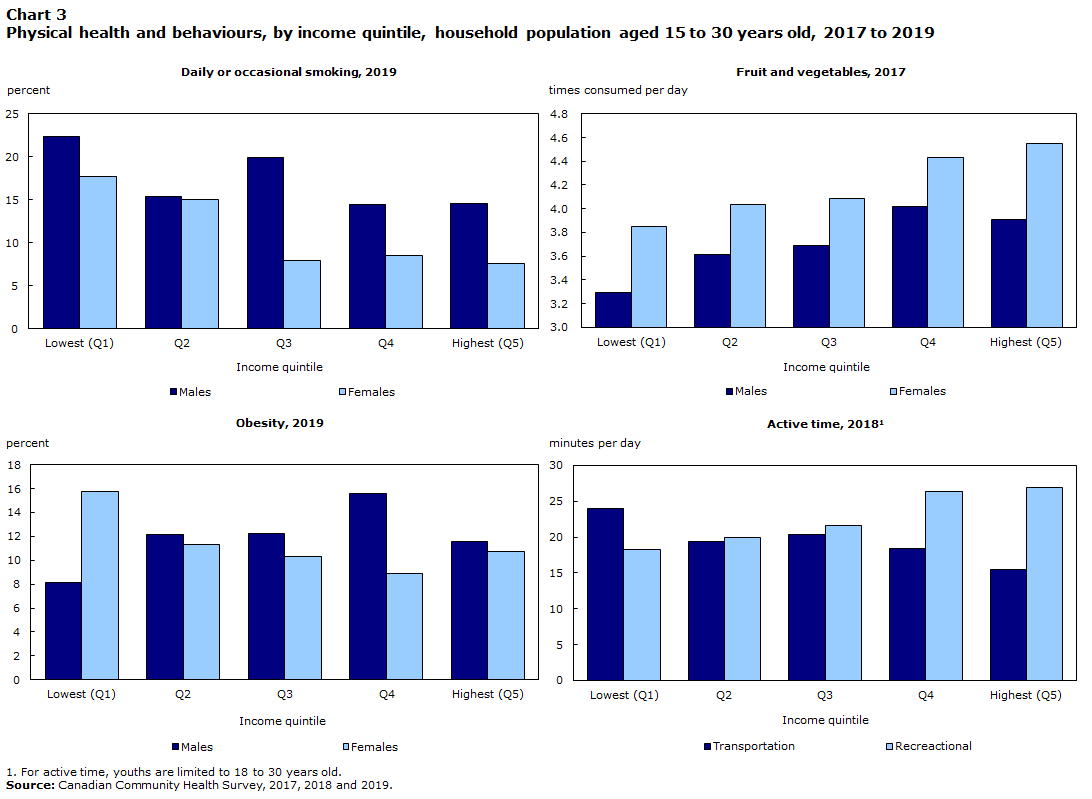
Youth living in households in the lowest income quintile had worse physical health and related behaviours than youth in higher-income households. For example, they were more likely to smoke cigarettes and less likely to eat fruit and vegetables. Despite spending more time during the day in active transportation than higher-income youth, they spent less time in recreational physical activity (Chart 3). Differences were more pronounced for young females, particularly for smoking.
Differences by visible minority status were also apparent in the physical health and behaviour indicators. Canadians who identified to groups designated as visible minorities smoked less and had lower obesity rates than White Canadians. This was also true when the smoking rates of only Black and White Canadians were compared (Chart 4).
Data table for Chart 3
| Income quintile | Daily or occasional smoking, 2019 | Fruit and vegetables, 2017 | Obesity, 2019 | Active time, 2018Data table Note 1 | ||||
|---|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | All | ||
| percent | times consumed per day | percent | minutes per day | |||||
| Lowest (Q1) | 22.3 | 17.7 | 3.3 | 3.9 | 8.1 | 15.8 | 18.3 | 24.0 |
| Q2 | 15.3 | 15.0 | 3.6 | 4.0 | 12.2 | 11.3 | 20.0 | 19.3 |
| Q3 | 19.9 | 7.9 | 3.7 | 4.1 | 12.2 | 10.3 | 21.6 | 20.4 |
| Q4 | 14.5 | 8.5 | 4.0 | 4.4 | 15.6 | 8.9 | 26.4 | 18.5 |
| Highest (Q5) | 14.5 | 7.6 | 3.9 | 4.5 | 11.6 | 10.7 | 27.0 | 15.5 |
|
||||||||
However, Canadians who identified to population groups designated as visible minorities spent less time, on average, doing recreational physical activity and ate fewer fruit and vegetables than White Canadians.
Self-perceived health has remained stable over the last 20 years for youth aged 15 to 30, while certain indicators, such as fruit and vegetable consumption, obesity, and physical activity, have not. Research on longevity, cardiovascular disease and cancer suggests that adopting less healthy behaviours at a relatively young age will affect people’s health over time. On a more positive note, improvement in youth smoking rates should have beneficial long-term consequences on the health of Canadians.
In 2019, 61% of youth in lower-income households reported excellent or very good health, 14 percentage points below youth in the highest-income households. Youth who belong to a population group designated as visible minority were more likely than White youth to report excellent or very good health (71%, compared with 67%).

Data table for Chart 4
| Visible minority status | Daily or occasional smoking, 2019 | Fruit and vegetables, 2017 | Obesity, 2019 | Recreational active time, 2018Data table Note 1 |
|---|---|---|---|---|
| percent | times consumed per day | percent | minutes per day | |
| Visible minority | 10.4 | 3.5 | 8.7 | 16.7 |
| Black Canadians | 5.8 | 3.4 | 12.0 | 15.2 |
| White | 17.2 | 4.1 | 13.4 | 20.5 |
|
||||
Mental health
Age and sex
Physically, young Canadians were in better shape than their older counterparts. But the story is different when it comes to mental health. Adolescence and young adulthood are marked by important changes, decisions and milestones, including studying for years, graduating, searching for a job, working on career development, relocating, finding a partner and starting a family. This can be a challenging time for some people.
Data table for Chart 5
| Age | Mental health | Lifetime Suicidal thoughts | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| percent | ||||
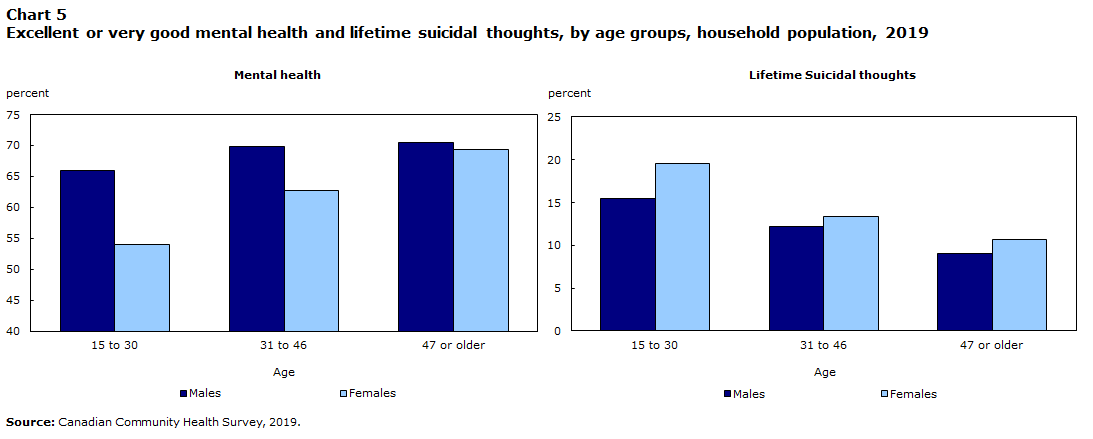
| 15 to 30 | 66.0 | 54.0 | 15.5 | 19.6 |
| 31 to 46 | 69.8 | 62.7 | 12.2 | 13.3 |
| 47 or older | 70.5 | 69.3 | 9.0 | 10.6 |
| Source: Canadian Community Health Survey, 2019. | ||||
In 2019, fewer Canadian youth than older Canadians reported having excellent or very good mental health. The difference was essentially driven by young females (Chart 5), who reported lower mental health than young males. In addition, youth aged 15 to 30 were more likely to report that they had seriously contemplated suicide in their life (Chart 5). This was true both for males and females, although young females reported having contemplated suicide more often than young males. However, males were actually more likely to die by suicide. The suicide rate of young males was 2.5 times higher than that of young females (16.9 per 100,000, compared with 6.6).
Start of text box
- In a survey conducted from March 19 to April 3, 2020,
- 48.7% of 15- to 30-year-old males reported excellent or very good mental health
- 32.4% of 15- to 30-year-old females reported excellent or very good mental health.
- In a survey conducted three months later, the percentage of males (44.3%) and females (33.0%) who reported excellent or very good mental health did not change.
- In data collected in a crowdsourcing project from April 24 to May 11, more than 6 in 10 participants aged 15 to 34 reported that their mental health had worsened since the onset of COVID-19 and related measures such as physical distancing. This proportion was higher than that in any other age group.
End of text box
Suicide rates differed little by age group (11.9 per 100,000 Canadians aged 15 to 29, compared with 11.5 for Canadians aged 30 to 44 and 12.5 for Canadians aged 45 or older).Note 7
One of the biggest impacts of COVID-19 and related public health measures such as physical distancing and school closures was on mental health. The impact on the mental health of youth was the largest of any age group. For example, according to data collected at the end of March and into the first week of April, 39.7% of youth aged 15 to 30 reported excellent or very good mental health, a 20% decrease compared with 2019.Note 4 Three months later, the mental health of young Canadians remained at this lower level.
The majority of youth aged 15 to 34 who completed a crowdsourcing survey at the end of April and in early May 2020 reported that their mental health had worsened since the beginning of physical distancing.Note 8
Longer-term trend
Self-reported mental health has not always been lower among youth than among older Canadians. This trend happened recently. In 2003, the percentage of Canadian youth reporting excellent or very good mental health was at its highest (76%) and very similar between males and females. Since then, it has been slowly decreasing, to 73% in 2013/2014 and to 60% in 2019 (Chart 6). The self-reported mental health of both males and females showed downward trends, but the decline for females has accelerated in the last 10 years. The spread between males and females went from 0.5 percentage points in 2003 to 4.2 percentage points in 2013/2014 and to 12.0 percentage points in 2019.
Suicide ideation has seldom been asked about in the last 20 years in Statistics Canada’s health surveys. The last time the question was asked was in 2015/2016. At the time, 14.5% of youth reported having contemplated suicide in their lifetime, 3 percentage points below what was reported in 2019. Going back further, in 2002, 12.0% of young Canadians reported “having seriously thought about committing suicide or taking their own life”.
While suicide ideation can be an important measure of mental health, completed suicides can be tracked and analyzed each year. Since 2000, suicide rates among youth aged 15 to 29 have been relatively stable. From 2000 to 2018, suicide rates averaged 11.4 per 100,000—the low was 9.8 in 2006, and the high was 13.1 in 2000. This represents an average of 775 deaths a year.Note 7 Although always higher in young males than females, suicide rates have been relatively stable for both sexes.

Data table for Chart 6
| Males | Females | All | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| 15 to 30 | 31 to 46 | 47 or older | 15 to 30 | 31 to 46 | 47 or older | 15 to 30 | 31 to 46 | 47 or older | |
| percent | |||||||||
| 2003 | 76.5 | 73.9 | 71.0 | 76.0 | 73.7 | 70.8 | 76.3 | 73.8 | 70.9 |
| 2005 | 77.5 | 75.4 | 72.7 | 76.4 | 74.3 | 71.8 | 77.0 | 74.9 | 72.2 |
| 2007 to 2008 | 78.1 | 77.2 | 72.1 | 76.7 | 73.4 | 71.7 | 77.4 | 75.3 | 71.9 |
| 2009 to 2010 | 78.0 | 75.9 | 71.6 | 76.5 | 72.8 | 71.2 | 77.2 | 74.3 | 71.4 |
| 2011 t0 2012 | 76.1 | 73.5 | 70.7 | 74.3 | 70.6 | 69.2 | 75.2 | 72.1 | 69.9 |
| 2013 to 2014 | 74.7 | 72.9 | 69.6 | 70.5 | 70.1 | 69.4 | 72.7 | 71.5 | 69.5 |
| 2015 to 2016 | 74.2 | 74.9 | 72.1 | 67.0 | 69.8 | 69.9 | 70.7 | 72.3 | 71.0 |
| 2017 to 2018 | 70.6 | 72.4 | 71.6 | 60.2 | 66.5 | 69.4 | 65.5 | 69.4 | 70.5 |
| 2019 | 66.0 | 69.8 | 70.5 | 54.0 | 62.7 | 69.3 | 60.2 | 66.2 | 69.9 |
| Source: Canadian Community Health Survey, 2003 to 2019. | |||||||||
Social determinants
Income was associated not only with physical health but also with mental health. Youth living in the poorest households were less likely to report excellent or very good mental health and more likely to report having seriously contemplated suicide in their lifetime (Chart 7).

Data table for Chart 7
| Income quintile | Mental health, 2019 | Suicidal thoughts 2019 | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| percent | ||||
| Lowest (Q1) | 58.7 | 49.5 | 17.5 | 23.6 |
| Q2 | 68.1 | 52.4 | 14.7 | 24.1 |
| Q3 | 62.5 | 58.6 | 17.1 | 16.1 |
| Q4 | 70.2 | 57.0 | 13.9 | 15.8 |
| Highest (Q5) | 72.1 | 53.9 | 13.7 | 16.8 |
| Source: Canadian Community Health Survey, 2019. | ||||
No difference was observed in self-perceived mental health by visible minority status. Black Canadians, Canadians belonging to other population groups designated as visible minorities and White Canadians all had similar mental health levels. However, suicide ideation was lower for Canadians who belonged to groups designated as visible minorities than for White Canadians (12.9%, versus 19.9%), especially for females (12.8%, versus 23.2%). Suicide ideation for Black Canadians specifically was even lower, at 10.0%.
Substance use
Age and sex
People use alcohol and drugs for a variety of reasons, including to relax, have fun or experiment. Some also use alcohol and drugs to cope with problems, deal with negative feelings or even to overcome boredom.
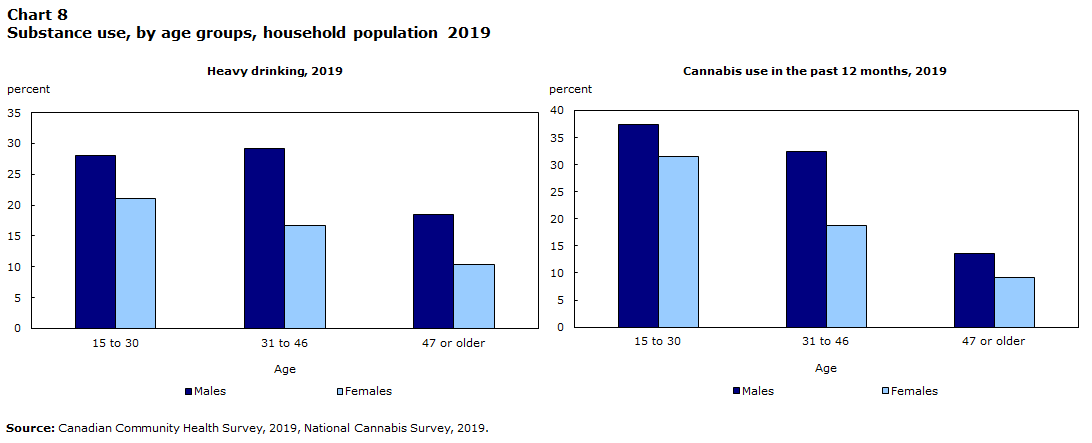
Heavy drinking is defined as consuming at least five drinks for a male and four drinks for a female on a single occasion at least once a month.Note 9 In 2019, Canadians aged 15 to 30 were more likely than older Canadians to be heavy drinkers (Chart 8).
Data table for Chart 8
| Age | Heavy drinking, 2019 | Cannabis use in the last 12 months, 2019 | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| percent | ||||
| 15 to 30 | 28.0 | 21.1 | 37.4 | 31.5 |
| 31 to 46 | 29.1 | 16.7 | 32.5 | 18.8 |
| 47 or older | 18.5 | 10.4 | 13.6 | 9.1 |
| Source: Canadian Community Health Survey 2019, National Cannabis Survey, 2019. | ||||
The legalization of non-medical cannabis use in October 2018 increased the need for monitoring, to understand the impact of legalization. In 2019, Canadians aged 15 to 30 were more likely than older Canadians to have consumed cannabis in the past 12 months (Chart 8).
According to data collected from March 19 to April 3, 2020 (corresponding to the beginning of the COVID-19 pandemic), most people did not report a change in their alcohol consumption or cannabis use.Note 10 However, youth aged 15 to 34 reported that they had increased their cannabis use. People with fair or poor mental health were also more likely to have reported an increase in cannabis use or alcohol consumption at the beginning of the pandemic period.
Start of text box
In a survey conducted from March 19 to April 3, 2020,
- 11.6% of 15- to 34-year-olds reported an increase in cannabis use (higher than any other age group)
- 18.7% of 15- to 34-year-olds reported an increase in alcohol consumption (comparable to 35- to 64-year-olds and more than the 65 and older age group).
Three months later, at the end of July 2020, the situation remained the same.
End of text box
Longer-term trend
Heavy drinking has decreased among young males in the last 15 years, from a high of 40% in 2005 to a low of 28% in 2019 (Chart 9). The trend for females is more difficult to interpret. First, from 2001 to 2011/2012, heavy drinking increased from 16.5% to 23.2% for females. During these years, heavy drinking was defined as at least five drinks in one occasion, at least once a month. In 2013/2014, the number of drinks for females to be considered heavy drinkers was reduced from five to four. While the percentages did not change after that, the threshold for the definition of heavy drinking did change. A redesign in the methodology of the survey in 2015/2016 made comparisons even more difficult. In all likelihood, heavy drinking among young females has increased over the last 20 years.

Data table for Chart 9
| Heavy drinking | ||
|---|---|---|
| Males | Females | |
| percent | ||
| 2001 | 34.7 | 16.5 |
| 2003 | 38.5 | 18.9 |
| 2005 | 39.6 | 20.1 |
| 2007 to 2008 | 37.9 | 21.3 |
| 2009 to 2010 | 38.4 | 21.0 |
| 2011 to 2012 | 38.4 | 23.2 |
| 2013 to 2014 | 33.8 | 23.5 |
| 2015 to 2016 | 31.7 | 23.6 |
| 2017 to 2018 | 30.3 | 23.1 |
| 2019 | 28.1 | 21.2 |
|
Note: Heavy drinking definition changed for women from 5 to 4 drinks a day in 2013 to 2014. Source: Canadian Community Health Survey, 2001 to 2019. |
||
For cannabis use, there was no change in use by youth aged 18 to 24 in the months preceding and following legalization.Note 11 Use among youth aged 15 to 17 appears to have dropped with legalization. Longer time-trend analysis also shows that past-year cannabis use had been decreasing among youth aged 15 to 17 between 2004 and 2017 but did not change for youth aged 18 to 24.Note 12
Social determinants
In 2019, heavy drinking was less frequent among youth identifying to groups designated as visible minorities, including Black Canadians, than among White Canadian youth. Contrary to most of the other health indicators presented here, heavy drinking was positively correlated with household income. Youth living in higher-income households consumed more alcohol than youth living in lower-income households (Chart 10).

Data table for Chart 10
| Income quintile | Heavy drinkning by income quintile | Cannabis consumption in the past 12 months by income quintile | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| percent | ||||
| Lowest (Q1) | 21.6 | 17.1 | 34.1 | 30.7 |
| Q2 | 23.9 | 21.6 | 32.8 | 32.5 |
| Q3 | 26.3 | 19.5 | 38.9 | 31.8 |
| Q4 | 31.8 | 23.4 | 39.5 | 31.5 |
| Highest (Q5) | 38.1 | 25.7 | 42.0 | 30.9 |
| Heavy drinking by visible minority status | Cannabis consumption in the past 12 months by visible minority status | |
|---|---|---|
| All | ||
| percent | ||
| Visible minority | 16.2 | 23.3 |
| Black Canadians | 19.7 | 25.5 |
| White | 29.4 | 40.6 |
| Source: Canadian Community Health Survey, 2019. | ||
The pattern was similar for cannabis use in the past 12 months. Young White Canadians were more likely than Black Canadians or Canadians identifying to a group designated as visible minority to report having used cannabis. Young Canadians living in higher-income households, particularly young males, were also more likely than youth living in lower-income households to report having used cannabis in the past 12 months (Chart 10).
Start of text box
A discussion of substance use in Canada must include opioid-related harms. The opioid overdose crisis is affecting every province and territory, and communities big and small. In the months following the emergence of COVID-19, the number of opioid-related deaths increased, according to some preliminary provincial reports.Note 13 Note 14
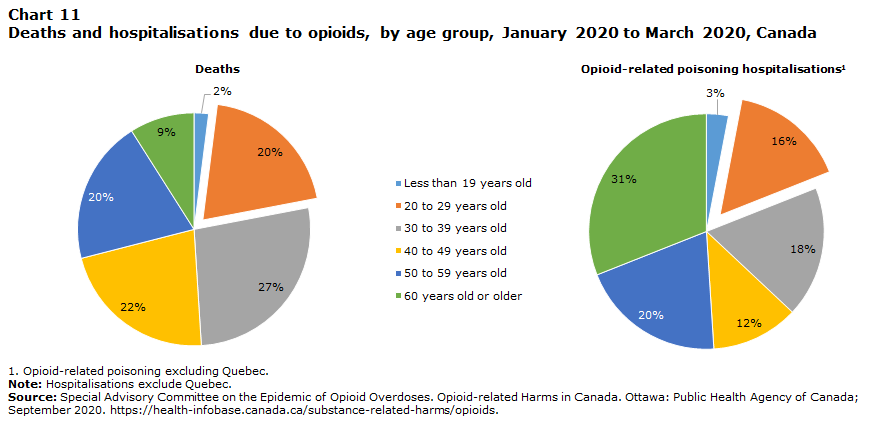
Youth are disproportionally represented in opioid-related deaths and hospitalizations for opioid-related poisoning. From January to March 2020, 1,018 opioid-related deaths and 1,067 opioid-related poisoning hospitalizations occurred in the country (excluding Quebec). People aged 20 to 29 years old represented 20% of the deaths and 16% of the hospitalizations, while accounting for 12.9% of the entire Canadian population.Note 15
Data table for Chart 11
| January 2020 to March 2020 | ||
|---|---|---|
| Deaths | HospitalisationsData table Note 1 | |
| Less than 19 years old | 2% | 3% |
| 20 to 29 years old | 20% | 16% |
| 30 to 39 years old | 27% | 18% |
| 40 to 49 years old | 22% | 12% |
| 50 to 59 years old | 20% | 20% |
| 60 years old or older | 9% | 31% |
| Total number | 1018 | 1067 |
Source: Special Advisory Committee on the Epidemic of Opioid Overdoses. Opioid-related Harms in Canada. Ottawa: Public Health Agency of Canada; September 2020. https://health-infobase.canada.ca/substance-related-harms/opioids. |
||
From 2013 to 2017, hospitalizations increased faster among Canadian youth than older age groups—they rose 53% among youth aged 15 to 24 and 63% among people aged 25 to 44.Note 16
It was not possible to analyze opioid-related hospitalizations by income level and other social determinants for youth specifically. However, data from 2011 to 2016 suggest that in the general population, opioid-related hospitalizations were much higher among White Canadians compared with Canadians identifying as part of a visible minority group (age-adjusted rate of 13 per 100,000, versus 2.9) and among people living in the lowest-income households (25.8 per 100,000) compared with those in the highest-income households (6.6 per 100,000).Note 17
End of text box
Conclusion
Canadian youth reported that they were in good overall health. They were in better physical shape than older Canadians but experienced considerably worse mental health. Some trends can be seen over the last two decades: obesity rates increased, while physical activity, fruit and vegetable consumption, and mental health were all in decline. The mental health of Canadian youth was at an all-time low, particularly during the pandemic.
On the other hand, smoking, heavy drinking and cannabis use were either stable or decreasing.
Canadians aged 15 to 30 identifying to a group designated as visible minority, particularly Black Canadians, were often doing better than White Canadians: they were less likely to smoke, use cannabis or drink heavily, and their obesity rates were lower. However, some health behaviours, such as physical activity and fruit and vegetable consumption, were lower than what was observed for White Canadians.
The biggest health and health behaviour differences were observed in households in the lowest income category. Young Canadians living in households in the lowest income quintile were more likely to smoke, ate fewer fruit and vegetables, and had less recreational physical activity than their wealthier peers. Fewer reported excellent or very good mental health, and higher numbers reported having contemplated suicide. More positively, fewer young Canadians living in the lower-income households reported heavy drinking than youth from higher-income households.
Of course, the information presented here is a sample of many characteristics of Canadian youth. Information about specific health conditions (e.g., asthma, diabetes, injuries and food insecurity) and health behaviours (e.g., screen time, time spent receiving support from or providing support to family and friends, and other dietary habits) should also be considered. For example, diabetes has increased among youth over the last 20 years; food insecurity affected one in six Canadian youth in 2017/2018, more than any other age group; and lower soft drink consumption reduced the sugar intake of Canadian youth compared with 2004.
Some health indicators, such as lower mental health, were affected in the short term by COVID-19 and the measures taken to limit its spread. Some people expect a shift in the coming months, and Statistics Canada will continue to monitor the recovery. Some health-related impacts of COVID-19 are also expected to be observed in the coming years. For example, surgical delays, preventive care and diminished access to regular doctor visits could influence the health of young Canadians in the future.
Start of text box
Data sources
Most of the data highlighted in this chapter come from various cycles of the Canadian Community Health Survey (CCHS). The CCHS is a cross-sectional survey that collects information related to health status, health care utilization and health determinants for the Canadian population. It was first conducted every two years (2001, 2003 and 2005) before moving to annual collection in 2007. A major redesign took place in 2015, including changes to the survey sampling and collection strategy.
The CCHS collects data from people aged 12 and older living in private dwellings. The sampling frame excludes individuals living on Indian reserves and Crown lands, institutional residents (health institutions, prisons, religious institutions, etc.), full-time members of the Canadian Forces, youth aged 12 to 17 living in foster homes, and residents of certain remote regions. The CCHS covers approximately 98% of the Canadian population aged 12 and older.
Definitions
Excellent or very good self-perceived general health: Respondents answered excellent or very good to the question “In general, would you say your health is... ?”
Smoking (daily or occasionally): This includes respondents who answered “daily” or “occasionally” to the question “At the present time, do you smoke cigarettes every day, occasionally or not at all?” “Daily” was replaced by “every day” starting in 2015.
Obesity: Obesity is based on self-reported height and weight. A body mass index (weight in kilograms divided by the square of height in metres) equal to or above 30 is classified as obese for respondents aged 18 or older. The World Health Organization thresholds by age and sex were used for respondents aged 15 to less than 18 years old to define obesity. Pregnant females were excluded.
Active time (transportation): Respondents who reported having used active ways such as walking or cycling to get to places such as work, school, the bus stop or the shopping centre or to visit a friend in the last seven days were asked “How much time in total, in the last 7 days, did you spend doing these activities? Please only include activities that lasted a minimum of 10 continuous minutes.” Questions were asked only to respondents aged 18 years or older from 2015 to 2018.
Active time (recreation): Respondents who reported having participated in the last seven days in sports, fitness or recreational physical activities, organized or non-organized, that lasted a minimum of 10 continuous minutes and that made them sweat at least a little and breathe harder were asked “How much time in total did you spend doing these activities that made you sweat at least a little and breathe harder?” Questions were asked only to respondents aged 18 years or older from 2015 to 2018.
Fruit and vegetables: Respondents were asked how many times they consumed the following products over the last month: 100% pure fruit juice, fruit, dark green vegetables, orange-coloured vegetables, non-deep-fried potatoes, and other vegetables. The sum of these products (with or without juice) was used to derive the average number of times consumed a day. Questions were only asked from 2015 to 2017.
Excellent or very good self-perceived general mental health: Respondents answered excellent or very good to the question “In general, would you say your mental health is... ?” The question was first asked in 2003.
Lifetime suicidal thoughts: Respondents answered yes to the question “Have you ever seriously contemplated suicide?”
Heavy drinking: Respondents answered at least once a month to the question “How often in the past 12 months have you had 5 (for males) or 4 (for females) or more drinks on one occasion?” Prior to 2013, the question referred to five drinks for all respondents.
Cannabis use in the past 12 months: Respondents answered yes to the question “Have you used cannabis in the past 12 months?” The question was new in 2019.
Income quintile: Residents of each province were distributed in quintiles (five categories including approximately the same percentage of residents for each province) based on the value for the adjusted ratio of their total household income to the low-income cut-off corresponding to their household and community size. This provides, for each respondent, a measure of their household income relative to the household incomes of all other respondents in the same province.
Respondents were asked about their cultural or racial background. Respondents who self-identified only as White were classified as White. Respondents who self-identified as Black were classified as Black. Respondents who were not White were classified as belonging to groups designated as visible minorities. Respondents who self-identified as an Aboriginal person, that is, First Nations, Métis or Inuk (Inuit), were excluded from these categories.
Methods
Weighted frequencies and cross-tabulations were calculated to examine the various indicators. Bootstrap weights were used to take into account the complex survey design when estimating the variance. Differences presented in the text were t-tested, and significant differences were identified at the p < 0.05 level.
Trends prior to 2015 are indicative only. Because of the changes made to the CCHS methodology in 2015, comparisons with previous years are not recommended.
End of text box
- Date modified: